
Bence Szabó Gál
Professional leader
Whatever form of vitamin B12 is consumed, although it enters the bloodstream in unchanged form, each form is broken down into cobalamin in the cells, and even the ligand (the adenosyl or methyl group) that is cleaved from the coenzyme forms is not used to produce the subsequent coenzyme form in the cell, i.e. no matter what form is ingested, it is broken down into cobalamin in the cells before the target form (the active B12 coenzyme form) is produced, so it is clear from the metabolism of the B12 forms that the form of cobalamin (B12) ingested does not matter.
This is also confirmed by human clinical studies where the utilisation/effects of different forms have been investigated. There is no significant difference, and it can vary from person to person which form is better for which person (often cyanocobalamin), but there is no significant difference; in the case of a rare genetic defect the hydroxocobalamin form is better absorbed than the adenosyl and methylcobalamin forms, but in general it doesn't matter which form you take. In addition, the hydroxocobalamin form has the added benefit of helping to eliminate cyanide, as cyanocobalamin is a natural metabolite in the body: The hydroxocobalamin in our diet is converted to cyanocobalamin when it meets the cyanide in our body, i.e. cyanocobalamin is a natural form of cyanide excretion. Of course, you can be scared by cyanide, but the average person's diet contains about 100-1000mcg of cyanide per day, while it is recommended to take about 100-300mcg B12, which, taken as cyanocobalamin, contains about 2-6mcg of cyanide, calculated at 2% cyanide, which is a fraction when compared to our average daily intake of cyanide from natural foods. Even 1 tablespoon of flaxseed contains more than 1000 mcg of cyanide. However, I also prefer the methylcobalamin form, just to be on the safe side. The other forms are also good, but only cyanocobalamin and methylcobalamin have a wide range of raw materials available from manufacturers here in the EU, and therefore, base materials with reliable quality for these two forms are easy to find.
All forms of B12 are equally good, although hydroxocobalamin may have some advantages over the others, but this is offset by its poor stability. Despite its bad reputation, cyanocobalamin is perfectly good. However, I primarily stilI recommend the methylcobalamin form, but they are all equally good. The active forms of coenzyme produced in the body are produced in the same proportion when each form is ingested, and this is not affected as they are all broken down into cobalamin in the cells before being used.
Utilisation of different forms of vitamin B12
I have drawn from 2 of the most recent papers published on the metabolism, utilisation and comparison of the different forms of B12, which are the most complete literature reviews on this topic to date.
One of them was published in 2015 and deals mainly with the utilisation of different forms. The title is: "The coenzyme forms of B12 (adenosyl and methylcobalamin) do not appear to be better than the cyano- and hydroxocobalamin forms in the prevention and treatment of vitamin B12 deficiency." [1]
And the other article [2] is from 2017, with the title: "Comparison of the different forms of B12 in supplements in terms of their absorption, utilization and properties that bridge genetic polymorphisms." It covers 3 topics. These (and their finding in a nutshell, in brackets) are as follows:
The exact pathway of metabolism/utilisation of the B12 forms used in the body. (They are utilized through the same or similar pathway, all are broken down into cobalamin once in the cells, so ultimately there is no difference: they produce the active coenzyme forms of B12 in the same proportion and potency)
Does either form have an advantage over the other for the average person, or for a specific genetic polymorphism? (It is unknown yet. However, the article from 2015 mentions a case where hydroxocobalamin may be preferable to other forms in very rare genetic defects)
Misconceptions about different forms of B12 and methylation. (Taking methylcobalamin does not enhance methylation any more than taking any other form, because the methyl group is broken down much earlier, and the methyl group that gives methylcobalamin its methylation ability from cobalamin inside the cell is not from the ingested/administered methylcobalamin, but from SAMe or methylfolate involved in the cellular cycles, i.e. whichever form is taken, they have the same effect on methylation)
Occurrence and functions of vitamin B12
Vitamin B12 (cobalamin, Cbl) is found in foods in the form of hydroxocobalamin (OHCbl), methylcobalamin (MeCbl) and adenosylcobalamin (AdCbl) (and some other forms). Eggs and dairy products have more MeCbl, while meats have slightly more of the AdCbl form than the others. [1,2] Cyanocobalamin (CNCbl) is almost non-existent in food, it is just a natural metabolite in our body that is formed during the detoxification of cyanides from food.
MeCbl, AdCbl and a newly discovered cobalamin coenzyme, glutathionylcobalamin (GSH-Cbl), which is a form of cobalamin formed by reduced glutathione and plays an important role in nitric oxide production, are also produced in our cells as cofactors. These are the 3 known coenzyme forms of cobalamin (B12). OHCbl and CNCbl are not coenzymes in the body. The former is abundant in our foods, the latter is mostly only naturally formed in us, and is only present in trace amounts in our foods, unless fortified. Of the 5 forms, only GSH-Cbl is not used in supplements. CNCb is most commonly used, as it is the most stable, most tested and by far the cheapest. MeCbl is also used, but less frequently, because it is much more expensive. OHCbl, although cheap, is quite unstable and thus rarely used, while AdCbl is very expensive, has no known advantages + the supply side of this raw material is quite unreliable. Well-known, reputable suppliers do not deal with it, so it requires serious scrutiny if a final product manufacturer wants to integrate it into their product and also wants to make sure that they have received a clean raw material. In my opinion, this is the reason why it is not used, because it is expensive and its scrupulous use would require constant regular and costly laboratory testing, while it has no known or suspected benefit based on literature and physiological knowledge.
Not much difference between the various forms
Whichever form we consume, they eventually reach our cells, where they are broken down into cobalamin before being used, and then produced within the cell to form the active coenzyme B12.[2] In the mitochondria, cobalamin is given an adenosyl group to form the coenzyme AdCbl, while in the cytosol it is given a methyl group to form the coenzyme MeCbl. [2] There is also a form of coenzyme called GSH-Cbl and possibly other forms of coenzyme that are not yet known. The efficiency of the formation of these forms of coenzyme and the rate of their formation is not affected by the B12 form that enters the cells, because they are all broken down into cobalamin before they are used, i.e. it is in vain to ingest e.g. AdCbl or MeCbl, since their adenosyl or methyl groups are broken down by enzymes within the cell and only the cobalamin is used within the cell in the cytosol and mitochondria to produce the active forms.[2] The cleaved groups are also not reused in their forming, so taking coenzyme forms directly do not even offer this advantage.[2] Whether we consumed CNCbl, ADCbl , MeCbl , or OHCbl, the same amount of AdCbl, MeCbl and GSH-Cbl will be produced in our body, i.e. in our cells. It is conceivable that in some people particular doses of one form or another may be better or less effective, or have higher or lower retention, but even so there is no significant difference + even if there were, it is impossible to decide which form would be preferable. [2] There are only two specific cases where one form clearly stands out from the others:[1] OHCbl is better absorbed in a very rare genetic defect (there is only one documented case in a single infant) than AdCbl or MeCbl. In addition, in the case of cyanide poisoning, high doses of OHCbl are also useful, as it will certainly convert to CNCbl when it encounters cyanide, thereby neutralising the cyanide (although this property is presumably also present in other forms of B12, at least my understanding is that it is due to cobalamin itself, but I didn't think it was important enough to look into it further, so I can only say for sure for OHCbl)
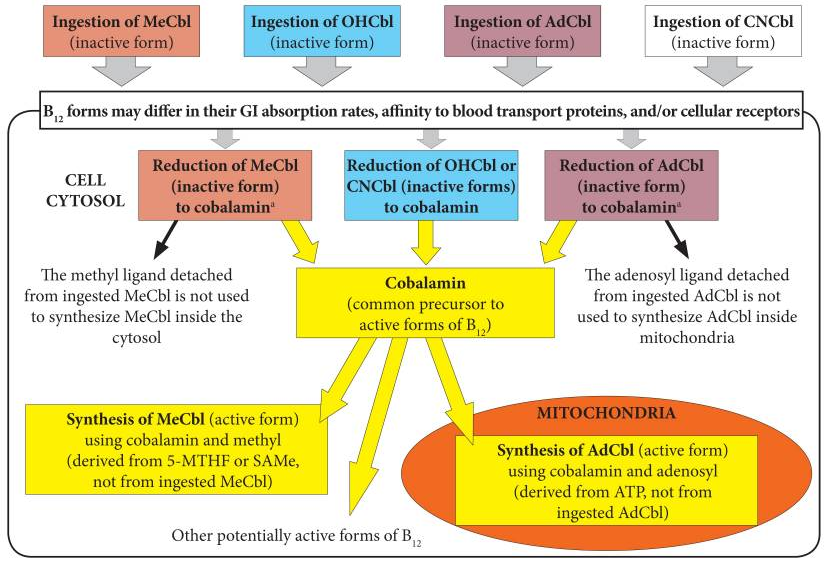
(Source: 2. reference)
Why is vitamin B12 utilized better from supplements than from food?
It is also important to note that strong stomach acid is not required for the absorption of vitamin B12 from supplements, only B12 ingested through diet. In our natural foods, vitamin B12 is part of a protein matrix that is first broken down by stomach acid and then transported to the small intestine by B12 bound to another protein. Within the small intestine, protein-degrading enzymes are required to allow it to be eventually absorbed by binding to IF or, at the right concentration, to be absorbed by diffusion, but this requires a concentration that can only be provided by supplements. Many digestive problems can lead to a reduction in the production of enzymes and proteins needed to absorb B12, and low stomach acid can also lead to vitamin B12 deficiency in the long term. The advantage of B12 supplements is that they are not bound to a protein matrix, so they do not require stomach acid for absorption, and their concentration allows them to be absorbed by diffusion, so they can also be used to meet B12 requirements in the case of the digestive problems mentioned above. B12 supplements include oral sprays and lozenges, which are intended to allow B12 absorption through the mucous membranes of the mouth, but it is not known exactly how much B12 can be absorbed in this way, probably immediately bound by saliva and then absorbed in the small intestine in the same way as other B12 preparations. This is backed up by two studies that have looked at exactly this topic, and found capsule supplements to be just as effective as the varieties dissolved in the mouth. [2]
Should we be concerned about the cyanocobalamin cyanide content?
Finally, a few words about cyanide, i.e. why the scare about cyanocobalamin cyanide content seems to be a (marketing?) scare tactic:
Cyanocobalamin contains less than 2% of cyanide by weight. The average healthy person weighing 70kg has a detoxification rate of 4,200 mcg of cyanide per hour, [3] this is the amount of cyanide causing no problem. That's nearly 100,000 mcg per day, or the equivalent of 5 million mcg of cyanocobalamin per day.
The average daily intake of cyanide for the average person from natural foods is around 50-1000 mcg, but can be much higher. Now, the cyanide part of cyanocobalamin is only less than 2% of the mass of cyanocobalamin, which means that 100 mcg of cyanocobalamin is only 2 mcg of cyanide intake, so even 1000 mcg of B12 in cyanocobalamin form is only 20 mcg of cyanide. The average low-cyanide daily meal contains about 10-100 times as much cyanide. A tablespoon (10g) of flaxseed, for example, contains about 2000 mcg of cyanide, or 100.000 mcg of cyanocobalamin... Well, it doesn't seem dangerous... I feel like the methylcobalamin lobby has also misled me so far. But I don't mind, because it doesn't make the product much more expensive, and since there is such a huge CNCbl resistance from the consumer side to this scaremongering, hardly anyone would buy it, it would be hard for it to benefit the consumer if no one bought it…
In summary
For the vast majority of people, all forms of B12 are equally good and equally effective, while for presumably about 99.9% of people, if there is a slight difference in absorption, it is not significant, while the effect is the same, since the same proportion of the different active B12 cofactors are produced in anyone. If you eat a lot of cyanide-containing foods (marzipan, almonds, apricot kernels, tapioca/cassava/manioc, yam, flaxseed, etc.) or you smoke (which also contains cyanide), you should probably choose hydroxocobalamin and avoid cyanocobalamin out of precaution. Methylcobalamin is my preferred choice because it has a good quality supply of raw materials and although it is many times more expensive than cyanocobalamin, it is still inexpensive and, unlike cyanocobalamin, it is one of the main forms found in food. While there may be no advantage of either one over cyanocobalamin, I always keep realistic view in mind, and taking more than a few mcg of B12 in the form of cyanocobalamin is not realistic, while the other forms are. There is nothing wrong with it, but just in case…
-
Obeid, Rima et al. “Cobalamin coenzyme forms are not likely to be superior to cyano- and hydroxyl-cobalamin in prevention or treatment of cobalamin deficiency.” Molecular nutrition & food research vol. 59,7 (2015): 1364-72. doi:10.1002/mnfr.201500019
-
Paul C, Brady DM. Comparative Bioavailability and Utilization of Particular Forms of B12 Supplements With Potential to Mitigate B12-related Genetic Polymorphisms. Integr Med (Encinitas). 2017;16(1):42-49.
-
Evaluation of the health risks related to the presence of cyanogenic glycosides in foods other than raw apricot kernels EFSA Panel on Contaminants in the Food Chain (CONTAM),Dieter Schrenk,Margherita Bignami,Laurent Bodin,James Kevin Chipman,Jesús del Mazo,Bettina Grasl-Kraupp,Christer Hogstrand,Laurentius (Ron) Hoogenboom,Jean-Charles Leblanc,Carlo Stefano Nebbia,Elsa Nielsen,Evangelia Ntzani,Annette Petersen,Salomon Sand,Christiane Vleminckx,Heather Wallace,Diane Benford,Leon Brimer,Francesca Romana Mancini,Manfred Metzler,Barbara Viviani,Andrea Altieri,Davide Arcella,Hans Steinkellner,Tanja Schwerdtle First published: 11 April 2019 https://doi.org/10.2903/j.efsa.2019.5662