
Bence Szabó Gál
Professional leader
Pantethine, a vitamin B5 analogue not found in our foods, is 10x more expensive but at most as good as regular pantothenic acid/pantothenate (e.g: Ca-pantothenate), because when taken orally it is 100% converted to pantothenic acid before it enters the bloodstream, and its utilisation is less good than pantothenic acid (e.g: Ca-pantothenate). When used in pharmacological/supraphysiological (huge) doses, pantethine has effects that vitamin B5 does not have at any dose. However, these effects of pantethine are not due to its ability to convert to vitamin B5 or to its ability to raise the levels of the active coenzyme (CoA) formed from B5, i.e. not because it is a more "active" or more utilizable form of vitamin B5, but because it is broken down in the body into cysteamine. As a vitamin B5, the use of pantethine is in no way preferable to pantothenic acid. Thus, although pantethine has therapeutic effects other than vitamin B5 when used in supraphysiological/pharmacological doses, its use as vitamin B5 would only make sense as part of a nanocolloid system, or possibly injected, at maximum, in huge doses, as it is converted orally into pantothenic acid in the small intestine before it is absorbed into the bloodstream. The use of pantethine as a source of cysteamine without side effects is often effective (e.g. for cholesterol reduction), but it has no place in preparations as a source of vitamin B5. It's fine if they have such content, but it only makes them unnecessarily expensive, so it simply plays a marketing role.
Forms of vitamin B5 and their absorption
In foods, vitamin B5 is mainly present in the form of coenzyme A (CoA) and 4-phosphopantetheine, and only to a small extent in the form of pantetheine and pantothenic acid. [1,3,5,6] CoA is the ready-made, "most active" form of B5, i.e. it is the coenzyme itself, the final form of B5 that is formed in our cells. And 4-phosphopanthetin is the form 2 steps before CoA. So, similarly to vitamins B1, B2 and B3, we ingest vitamin B5 from our food mainly in the form that it will later be converted into in our cells, i.e. as a ready-made coenzyme. It's natural, because what we eat are also living things, and they have these vitamins in them because they need them (their cells) – they don't produce them for us, their cells use them in their ready-made forms. But we cannot use them directly, they do not just go from the cells of the food we eat into our cells. We first have to break them down in our digestive tract into their simplest forms so that they can pass through our intestinal cells into our bloodstream and then systemically to our cells in the bloodstream and into our cells. For B1, this is the form that can be absorbed/utilised/uptaken into cells: thiamine, for B2 riboflavin, for B3 niacin/niacinamide, and for vitamin B5 pantothenic acid/pantothenate. So, first we break down the finished form into the most primitive/simplest/smallest form, so that it can get to and into our cells, where it is then rebuilt from the simplest form into the finished form.
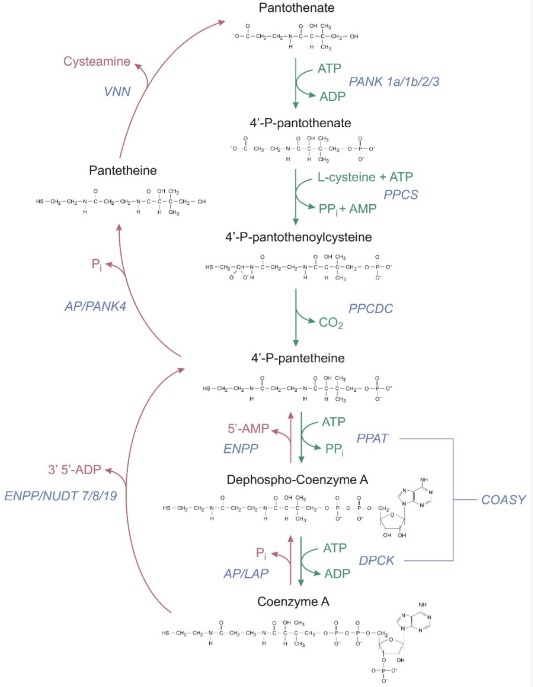
Image source: Reference number 1
Forms of vitamin B5 available in food supplements
In food supplements, vitamin B5 is usually used in the form of sodium or calcium pantothenate, which, when swallowed or dissolved in anything, immediately breaks down (dissociates) into sodium and calcium and pantothenic acid, respectively. Dexpanthenol is another form, but it has more of a place in creams, so I won't go into that. And pantethine is a newly approved form of vitamin B5, which is a virtually artificial analogue of vitamin B5, as it is not found in food. 2 pantetheine molecules form 1 pantethine molecule. Pantetheine is a form of vitamin B5 also found in food. After ingestion, pantethine is broken down in the small intestine into pantothenic acid (pantothenate) before being absorbed. [1,3,4,5,6] Some of it is already degraded to pantothenic acid in the small intestine by the abundantly present enzyme panteteinase, while some of it may be absorbed as pantothenic acid by intestinal cells if the dose is high and there is not enough enzyme in the intestinal lumen to convert it, but in this case it is the intestinal cells that break down the pantethine into pantothenic acid. [5,6] Finally, pantethine enters the bloodstream only when it is broken down into pantothenic acid. This has been studied in both humans and animals. In humans, even at extreme doses, pantethine (1000 mg/kg) has not been able to reach the bloodstream even in trace amounts, but only as pantothenic acid. [1,4] The utilisation of pantethine and Ca-pantothenate has been compared in another study. [6] Although the absorption of pantethine itself seems to be slightly better, it was excreted faster, so that in the end, even a 2x dose of pantethine increased the blood B5 level by only 18% more than the dose of Ca-pantothenate, which concluded that although pantethine also has a good uptake, it is less than or at most equal to Ca-pantothenate. [6]
Why pantethine is not better than pantothenic acid
It is clear from the above that pantethine used orally should not offer advantages over plain pantothenic acid, only a disadvantage in terms of increased CoA levels, i.e. in terms of the effect of vitamin B5. However, there have been human clinical trials where high oral doses of pantethine have been tested to see if they might be effective in increasing CoA levels in children with so-called PANK mutations. [2] It is a genetic problem where pantothenic acid cannot be converted by cells into active CoA, affecting one or two in a million people, and causing a neurological disease called PKAN. Treatment of midges with the PANK mutation using pantethine overcame this conversion problem, which is why it has been tried in humans. [2] I suppose it was easier to use orally and therefore is was not applied intravenously – although this is surprising to me – because they would have known from previous studies that there was no advantage to oral administration over plain Ca-panotenate. And really, there wasn’t:
Children with PANK defects were given 60 mg/kg of pantethine per day for six months (a very massive dose, 3600 mg/day for a 60 kg adult). The expected increase in CoA levels was not achieved and was lower at the end of the study than at the beginning. It is possible that it may have helped to mitigate the deterioration of their condition, i.e. it may have slowed the rate of decline in their CoA levels, but it was not the case for the simple pantothenic acid (e.g: Ca-pantothenate), since even in the presence of non-zero PANK enzyme deficiency, it was not only the conversion efficiency that ways poor.
Although, as a source of vitamin B5 (for CoA boosting), as we have seen, pantethine is no better and even slightly worse than e.g. Ca-pantothenate, it seems to be a very useful compound for other purposes, but only in huge pharmacological/supraphysiological doses, i.e. in the order of about 1000 mg per day. At this dose, it has a good effect on cholesterol and triglyceride levels, and everything else that the (natural) drug substance cysteamine does. Pantethine is effectively a prolonged absorption cysteamine, as the pantethine released from it is broken down into pantothenic acid and cysteamine. [1,4] Its action other than vitamin B5 is due to its breakdown into cysteamine. Although cysteamine is more effective than pantethine, for many people cysteamine is a drug with hard-to-tolerate side-effects, whereas pantethine is well tolerated by anyone with virtually no side effects. [4] Pantethine is an excellent drug for replacing cysteamine (e.g. in cases of cystine metabolism disorders) or for cholesterol control. However, when used as vitamin B5, it is only 10 times more expensive than the much studied Ca-pantothenate, but not even slightly better.
In summary
Pantethine should not be considered as a source of vitamin B5, because although it is a source of vitamin B5, using it for this purpose (to boost CoA levels) is a bit worse than the well-established Ca-pantothenate. It should be considered as a side-effect-free alternative to cysteamine. Used at a daily dose of around 1000 mg, it has a blood fat/cholesterol regulating effect, among other things. However, when used in lower doses, it only functions as a source of vitamin B5, but is slightly less good for that and about 10 times more expensive (Ca-pantothenate is inherently expensive, i.e. if it is replaced by pantethine in a product, its consumer price is unnecessarily and greatly increased).
-
Czumaj A, Szrok-Jurga S, Hebanowska A, Turyn J, Swierczynski J, Sledzinski T, Stelmanska E. The Pathophysiological Role of CoA. International Journal of Molecular Sciences. 2020; 21(23):9057. https://doi.org/10.3390/ijms21239057
-
Chang X, Zhang J, Jiang Y, Yao B, Wang J, Wu Y. Pilot trial on the efficacy and safety of pantethine in children with pantothenate kinase-associated neurodegeneration: a single-arm, open-label study. Orphanet J Rare Dis. 2020;15(1):248. Published 2020 Sep 14. doi:10.1186/s13023-020-01530-5
-
Yoshii K, Hosomi K, Sawane K, Kunisawa J. Metabolism of Dietary and Microbial Vitamin B Family in the Regulation of Host Immunity. Front Nutr. 2019;6:48. Published 2019 Apr 17. doi:10.3389/fnut.2019.00048
-
Wittwer CT, Gahl WA, Butler JD, Zatz M, Thoene JG. Metabolism of pantethine in cystinosis. J Clin Invest. 1985;76(4):1665-1672. doi:10.1172/JCI112152
-
National Institute of Health, Pantothenic acid Fact Sheet for Health Professionals
-
Scientific Opinion of the Panel on Food Additives and Nutrient Sources added to Food (ANS) on a request from the Commission on pantethine as a source for pantothenic acid added as a nutritional substance in food supplements. The EFSA Journal (2008) 865, 1-20.