
Bence Szabó Gál
Professional leader
The simplest forms of thiamine are the best
When consumed as a dietary supplement, the best form of vitamin B1 is plain thiamine (thiamine hydrochloride and thiamine mononitrate), while the intracellular active coenzyme form, TPP (along with TMP and TTP), is the least good form, as it must first be enzymatically degraded to plain thiamine before it can be absorbed at all. In the best case (if enough digestive and other enzymes are produced) it is only as good as free thiamine, in the worst case (if not enough enzymes are produced) TPP is not even utilized when taken orally.
Because supplements are not taken by our cells, vitamin B1 in the form of free thiamine is more likely to reach our cells as TTP than TTP taken orally. So, let's go through the different forms of B1 in foods and supplements, and then look at what happens to the different forms of B1 we consume and how they get into our cells.
The forms of vitamin B1 found in food and in our bodies are thiamine (free thiamine) and its phosphoesters, thiamine monophosphate (TMP), thiamine diphosphate or thiamine pyrophosphate (TPP) and thiamine triphosphate (TTP). In foods of animal origin, thiamine phosphoesters predominate, mainly TTP, while free thiamine is more abundant in plant source foods.
They are also found in food supplements, more specifically their salts, i.e. free thiamine in the form of thiamine hydrochloride and thiamine mononitrate, while TMP and TPP (no TTP) are in the form of TMP and TPP chloride.

Image source: the first reference
What happens after we swallow them?
In foods, free thiamine and thiamine phosphoesters are released from binding to food proteins during digestion and then they are present in the form of free thiamine, TMP, TPP and especially TTP in the small intestine, where they are all broken down to free thiamine by various enzymes.
For B1 from supplements, the situation is even simpler. Here, they do not need to be released from their protein-bound state, because, just as all salts in any liquid break down into their ions, so do they. After ingestion, thiamine hydrochloride is immediately converted (dissociated) in the stomach to free thiamine and hydrochloric acid, thiamine mononitrate to free thiamine and nitrate, and TMP and TPP chloride to TMP/TPP and chloride.
TMP and TPP cannot be utilized until after they are converted into free thiamine. This conversion to free thiamine (breaking the ester bond) is carried out by various non-specific enzymes, most notably an enzyme called alcaic phosphatase, which is found in our small intestine and many of our other tissues, as well as in our blood.
So whatever form of B1 we get, they are all converted to free thiamine in our small intestine. If something cannot be 100% metabolized in the absence of an enzyme, it cannot be utilized by TMP or TPP, so it passes on to the colon where it is consumed by bacteria. If the dose is high enough, it may be able to reach a special area of the colon where the cells of the colon may be able to take up TPP, although it will not enter the systemic circulation, but will only be a nutrient for the cells of the colon.
How does vitamin B1 get to our cells and into our bloodstream in the first place?
It is through our small intestine that B1 enters the systemic circulation, and it must first be converted to the free form of thiamine – if it is not in that form. This free thiamine is partially converted into TPP in the cells of our small intestine and then, because TPP cannot get out of the cells of the small intestine to enter the bloodstream, it is converted into TMP. So, from our small intestine, only free thiamine and TMP enter our bloodstream, and only these can reach our cells. Our cells can take up the free thiamine, whereas they have to convert TMP into free thiamine before they can take it up. Both TMP and thiamine are converted to TPP, TTP and TMP during entry into the cell and also inside the cell. TPP is the most important one – it is the form of coenzyme inside cells. There is no freely circulating TPP in our blood, only thiamine and TMP. TPP is found only inside cells (intracellularly).
So, in summary, in addition to the fact that our small intestine can only take up free thiamine and pass it on to the blood (partly converted into TMP), our cells are also able to only take up free thiamine. So the finished, active form of coenzyme B1 (TPP) is produced in our cells, so taking it in this form can't be an advantage, but it can be a disadvantage!
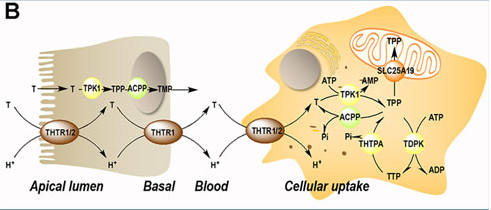
Image source: the first reference
Why is it disadvantageous to take B1 in its already active form in the cell, i.e. thiamine pyrophosphate (TTP)?
As already mentioned, enzymes have to convert TTP into free thiamine before it can be used, so it requires one more step from our body. Once it is converted into regular thiamine, it then follows the same course as if you took regular thiamine. Understandably, if you don't have enough digestive enzymes in your small intestine, especially if your alkaline phosphatase levels are insufficient, then you can assume that conversion is not taking place, in which case the unconverted part is not able to be utilized, at least not systemically. At best (and this is also very possible) it can provide some fuel for the cells in your colon, if the gut bacteria don't recover by then. In magnesium deficiency or when taking contraceptives, in diabetes, ischaemic heart/vascular disease, high cortisol levels or hypothyroidism, alkaline phosphatase levels are often insufficient, but digestive enzymes are also compromised in inflammatory bowel problems. In such cases, there is a risk that only the thiamine hydrochloride and mononitrate forms can be properly utilized, as they already provide free thiamine and no longer need to be converted.
The other problem is that the absorption of TPP is presumably inherently worse than that of plain thiamine, even in healthy people with high phosphatase enzyme levels, at least at sufficiently high intakes. Why? Although the absorption of plain (free) thiamine is not poor, with increasing intake (intestinal concentration), absorption becomes almost perfect, as it can be absorbed by passive transport at high intestinal concentrations, whereas at lower concentrations it can only be absorbed by various (less efficient) active transport proteins. If, however, we do not get ready-made thiamine, but its phosphoesters (e.g. TPP), which are wrongly called more bioactive, they must first become free, which enzymatic transformation delays the release of free thiamine in the intestines, i.e. the intestinal concentration cannot be as high as if we had ingested plain thiamine in the first place.
There is only one study comparing different forms of B1, and that was performed in pigs. They were given plant source foods that contain mainly thiamine, and those that contain mainly phosphate forms. They all had roughly the same utilization: utilisation rates of 77-94% were observed for foods rich in plain thiamine, while a slightly lower utilisation rate of 73-88% was observed for foods rich in "active" phosphate forms of B1. (Roth-Maier et al., 1999. Investigations on the intestinal availability of native thiamine in selected foods and feedstuffs. Eur. J. Nutr. 38, 241-246.)
What problems can consumers have when consuming products containing TPPs?
In various health conditions (inflammatory bowel problems, hypothyroidism, diabetes, cardiovascular disease, Zn/Mg deficiency, when taking contraceptives, in Wilson's disease, anemia, high cortisol level, etc.) the enzymes required for TPP to be utilized (converted to plain thiamine) are low, so for those for whom the B1 forms are intended to be active, they will be ineffective or at least certainly less effective than plain thiamine.
TPP is more expensive than thiamine, while at best only having the same effect -> money wasted
If the product developer mistakenly believes that TPP is a more bioactive form and therefore puts less in the product, then they have in fact put too little B1 in, while both they and the consumer are under the illusion that they are taking plenty of B1 when they are taking too little.
If someone wants to take high doses of B1 because they expect a change in condition, even in healthy people the uptake will be lower than for regular thiamine -> there may be no effect, leading the user and the practitioner to the wrong conclusion (for example, that the higher doses of B1 are not beneficial for the condition, although they would be, but they should not try the form they think is active.)
Proposed solution for direct delivery of ingested TPP to the cell
Since there is no way that the TPP we consume can get into our blood, let alone our cells, without being converted into thiamine, the only option is to inject the TPP directly into our cells (not enough into the blood). This is obviously unfeasible. However, when TPP is delivered as part of a nanocolloid system, e.g. encapsulated in unilamellar liposomes, niosomes or similar, around 200nm or smaller, they remain intact even when consumed orally and enter the cells, delivering TPP to its target site inside the cells. So we don't have to convert at all, and then back again. All this would be rather unnecessary, since there is no known condition in which plain thiamine cannot be properly converted into TPP. The exception is Mg deficiency, so we simply need to make sure that we are not Mg deficient. In any case, TPP can only be an advantage over plain thiamine as part of a nanocolloid system, in all other cases it is a disadvantage.
Summary
Whatever form of vitamin B1 we ingest will be converted into a form of plain thiamine in our intestines, without which it cannot be absorbed, and once it enters our bloodstream our cells can only absorb plain thiamine. So taking the intracellular active coenzyme form of vitamin B1 (TPP) orally is a waste of money at best, and at worst, it's useless. Why some manufacturers recommend the B1 form of TPP may be because they have forgotten that supplements are not taken by our cells, but by humans, in whom TPP can only reach the cells if it has first been broken down into plain thiamine. Oral administration of TPP is therefore one step further from the generation of intracellular TPP than oral administration of plain thiamine, and not one step closer.
-
Dhir, Shibani et al. “Neurological, Psychiatric, and Biochemical Aspects of Thiamine Deficiency in Children and Adults.” Frontiers in psychiatry vol. 10 207. 4 Apr. 2019, doi:10.3389/fpsyt.2019.00207
-
Yoshii, Ken et al. “Metabolism of Dietary and Microbial Vitamin B Family in the Regulation of Host Immunity.” Frontiers in nutrition vol. 6 48. 17 Apr. 2019, doi:10.3389/fnut.2019.00048
-
EFSA: Benfotiamine, thiamine monophosphate chloride and thiamine, pyrophosphate chloride, as sources of vitamin B1 added for, nutritional purposes to food supplements 1, Scientific Opinion of the Panel on Food Additives and Nutrient, Sources added to Food (ANS)(Question No EFSA Q-2005-128, EFSA Q-2005-093, EFSA Q-2005-164, EFSA Q-2006-261)Adopted on 24 September 2008
-
HEATON, F. Effect of Magnesium Deficiency on Plasma Alkaline Phosphatase Activity. Nature 207, 1292–1293 (1965). https://doi.org/10.1038/2071292b0
-
Sharma U, Pal D, Prasad R. Alkaline phosphatase: an overview. Indian J Clin Biochem. 2014;29(3):269-278. doi:10.1007/s12291-013-0408-y