
Bence Szabó Gál
Wissenschaftlicher Leiter
What if you found out that plain old vitamin K1 was just as good, maybe even better than the expensive K2, but it happens to be the best-kept secret? Are you familiar with Dumas' Iron Mask story, in which one of two twin princes is hidden in an iron mask while the other reigns supreme? Well, the situation with vitamin K is not unlike that: K1's iron mask is that it only regulates blood clotting and is well hidden from view. When found, it is claimed to be the result of some ill-conceived study... K1 has produced the effects of K2 in both animal and human studies, and in comparisons, it has beaten K2 hands down, yet we never hear about it... Nor do we hear that the modern western diet is actually very rich in K2 due to the consumption of processed industrial meat products, while the diet of indigenous peoples and our ancestors was practically devoid of K2, but had up to 100 times as much K1... Western people's K1 consumption has been reduced to a fraction and K2 has increased steeply in comparison to indigenous peoples and our ancestors...
Contrary to custom, I'll start my article with the summary and conclusion (practical recommendation), as I presume many people might not want to wade through the tedious details... Those who get curious about the details after the summary may continue reading under the summary table...
Summary and practical recommendations:
In principle, 500-1000 mcg of K1 of moderate to good absorption per day seems sufficient in the long run. For vegetable-derived K1, this means it should be eaten with sufficient fat and preferably heat-treated, while from supplements, an oil-soluble or emulsified form should be taken with meals so that absorption is around 80% and the half-life is rather long.
Some medicines (statins, bisphosphonates, coumarin derivatives) inhibit the conversion of K1 and MK-7 to K2 MK-4, so it is advisable to take MK-4 as well, at least 1500 mcg per day (after consulting your doctor.) D3, zinc, and magnesium enhance the conversion of K1 to K2. Vitamin A (retinol) and vitamin B6 also assist the effect of K2. It is worth minding sufficient consumption of these.
To preserve the natural MK4/K1 ratio in our tissues and thus enhance the effect of vitamins K and prevent counterproductivity, if you take K2 MK-7, you should also take at least 3x as much K1, while if you take MK-4 you should also take at least the same amount of K1 so that K2 vitamins do not cause any problems.
K1 is safe on its own, and unless its conversion is blocked by these drugs, K1 is the most potent of the K vitamins. Ideally, I recommend taking at least 500mcg of vitamin K1 daily in oil-soluble or emulsified form, but preferably 1000mcg. In addition to this, I also recommend optionally taking 100-200mcg of K2 MK-7, but no more. It may even be worth taking over 1000mcg of vitamin K1. 5mg a day seems ideal as in one study this amount (taken for 2-4 years) reduced cancer risk by a quarter and fracture risk by half.
| vitamin K1 (Phylloquinone) | K2 MK-4 (Menaquinone-4, or menatetrenone) | K2 MK-7 |
Other LC-MKs (MK-5-14) |
|
|---|---|---|---|---|
| Average Western consumption /day | 50-100 mcg | 20-100 mcg (mainly from processed industrial meat products) | 0-5 mcg (Japan: ~50 mcg) | 20-1000 mcg (mainly from processed industrial meat products) |
| Average content in health-conscious nutrition/day | 200-1000 mcg (from vegetables, olives, seeds and nuts, liver) | 5-10 mcg (low content in naturally raised meats) |
0-10 mcg (Japan: ~100 mcg) |
0-10 mcg (fermented vegetables and cheese, none in naturally raised meats) |
| Maximum consumption achievable with today’s foods and reasonable effort | Ca. 2500 mcg | Ca. 100 mcg (industrial meat products) | 200 mcg (natto) | 2000 mcg (industrial meat products) |
| Consumption in native people, as well as estimated consumption in the course of human evolution during the neolithic/ day |
Native peoples: ca. 1000 mcg or more Our ancestors: 1000 mcg – 1 million mcg |
10-100 mcg | Zero | Zero, unless consuming feces regularly |
| Absorption/biological utilization from whole foods | 10-80% (increased by cooking and addition of fats and oils | zero below 600 mcg, and around a third of that of K1 above 600 mcg | 75-100% | Presumably comparable to MK-7 |
| Absorption / biological utilization dissolved in oil or from emulsified nutritional supplements taken with fats and sufficient food | ~80% | zero below 600 mcg, and around a third of that of K1 above 600 mcg | 75-100% | Presumably comparable to MK-7 |
| Half-life if taken with food | ca. 6-7 hours | ca. 4 hours | Primary half-life 6-7 hours, secondary half-life 2 days | Similar to MK-7, but with an even longer secondary half-life |
| Occurrence and ratio in animal and human tissues | All tissues contain it. Bone, heart, and liver contain primarily K1. | Most tissues contain it. The brain, kidneys, arteries, and testes contain primarily MK-4 | Not naturally occurs in tissues, but the liver may store some. | Doesn't naturally occur in tissues, but the liver may store some. |
| Relative content in the body | Ca. 10-30% (the reason it is quite so low is that it is mostly converted to K3 in the course of absorption already, and then to MK-4 in the tissues. | Ca. 70-90% (All K vitamins are converted to MK-4 in the tissues, except for a contingent left purposefully in the form of K1) |
Ca. 0% (Unnecessary, therefore the body converts it to K3, then MK-4 for effectiveness)
|
Ca. 0% (Unnecessary, therefore the body converts it to K3, then MK-4 for effectiveness) |
| Is a large dose capable of upsetting the vitamin K balance in the tissues (K1/MK-4) | No | Slightly | Yes | Yes |
| How effectively does it activate clotting factors in the liver (there is no such thing as „overactivation", the goal is to activate all of it | Very well (ca. 100 mcg are sufficient for complete activation) | Capable of activation, but ineffective | Very well (ca. 30-40 mcg suffice for full activation | As well as MK-7, if not better |
| Effectivity in activating osteocalcin (a measure of the positive effect on the bones) | Very good (just 250 mcg activate nearly fully, 500-1000 mcg completely) | No effect below 600 mcg. 1500 mcg activate well, but even 45 thousand mcg MK4 do not activate as fully as 1000 mcg K1 | 90 mcg activate somewhat, but even high doses do not reach the effect of K1. | Not studied in humans |
| Effectivity in activating MGP (a measure of the positive effect on the cardiovascular system) | Very good: 500 mcg activate nearly fully (the highest activation measured) | No trials | Good, but surpassed by K1 | Unstudied |
| Effectivity in overall immune system benefit in epidemiological studies (more specifically in lowering all-cause mortality) | Yes (Over 400 mcg) | None (Only in studies that proved invalid) | None (Only in studies that proved invalid) | None (Only in studies that proved invalid) |
| Effectivity preventing CVD/CAC/CHD observed in epidemiological studies | Yes (over 400 mcg) | None (Only in studies that proved invalid) | None (Only in studies that proved invalid) | None (Only in studies that proved invalid) |
| Positive effect on the bones in epidemiological studies | Yes (over 400 mcg) | None | None (Only in studies that proved invalid) | None (Only in studies that proved invalid) |
| Positive effect on the bones proven in placebo-controlled studies | Yes, considerable (effects have been shown at doses ranging from 100-200 mcg, 500, 1000 to 5 thousand mcg) | Yes, considerable (At doses starting at 1500 mcg, but more so at doses around 45 thousand mcg) | Yes, in 100 and 180 mcg doses | Unstudied |
| Positive effect on the cardiovascular system proven in placebo-controlled studies | Yes, it was found to be effective in all RCT studies where it was examined. (3/3) | Not (3/0), or hardly effective: in a single study, it was found mildly effective, but only in mega doses in individuals gravely vitamin-K-deficient | Not really, in a subgroup of 1 study in a 180 mcg-os dose it was slightly effective, but not for the whole group, therefore ultimately ineffective in all studies | Unstudied |
| Placebo-controlled positive effect on coronary artery calcification | Yes, effective in multiple studies | Ineffective in all studies | Ineffective in all studies, in fact, it proved harmful in the most recent study at 360 mcg per day, as it increased calcification as compared to the placebo.s | Unstudied |
| Considerable effect in lowering cancer risk in placebo-controlled studies | Yes, taking it for 4 years at 2 mg per day lowered the risk of cancer by 75% | Yes, but only at doses exceeding 45 mg. | No | No |
| Effectiveness in preventing the progression/development of liver cancer proven in human interventional studies | Yes | Yes | No | |
| Ability to decrease the size of liver cancer in human interventional studies | Yes (50 participants, ca. 80% were stabilized or got better, tumor size decrease induced in many…) | No (though full remission was achieved in a study on leukemia patients) | No | No |
| Effectiveness when taken in nutritional doses? |
Yes |
No | Yes, but it appears counterproductive above 360 mcg (though doses over 200 mcg aren't realistic for normal nutrition, anyway) | Unstudied, but presumably similar to MK-7 once more. |
| Did they ever find counterproductive effects from its consumption in any human studies? | No, never. | Yes, in human as well as in preclinical studies. | Yes, in human as well as in preclinical studies. | Their effectiveness was never studied. |
| Overall effectiveness and safety. | Very effective on all points. Very safe at any dose. | Very effective for the bones, but not so much for the cardiovascular system. Safe, though the truly effective doses of 45 thousand mg/day have raised slight concern. | Effective for the bones, not so much for the cardiovascular system. Effective and fully safe up to a dosage of 200 mcg. 360 mcg are less effective and may be harmful. | Never studied, but may be similar to MK-7. |
| Prive of an effective dose | Pennies | Expensive |
Somewhat expensive |
As good as free. |
| Price /mg | 1x | 10x | 100x | 0,1x |
| Permitted in the EU? | Yes | No | Yes | No |
| Do statins, coumarins, and bisphosphonate-type medications inhibit its effect? | Yes | No | Yes | Yes |
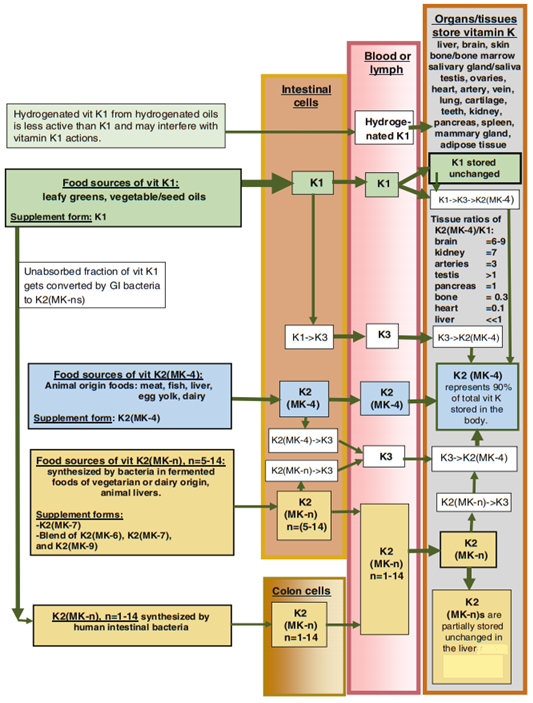
An excellent illustration of the transformation of vitamin K in the body from the chapter on vitamin K in the Pharmacology of Natural Medicines, 5th edition 2020 of the Textbook of Natural Medicines:
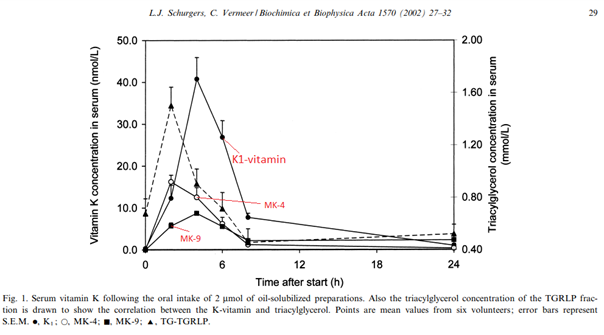
And a great chart showing the absorption of 900 mcg K1 + 900 mcg MK-4 + 1600 mcg MK-9 in a healthy person when consumed dissolved the butter of a breakfast toast:
The remaining reading time is about 75 minutes. We understand if you don't have the time or inclination to go into the topic in such depth, so we have also produced a 12-minute shortened version of the rest of the document, which you can read by clicking here.
(We have also removed the source links from the shortened version.)
Forms of vitamin K and their occurrence in nutrition
Vitamin K3 (menadione) - While it is not found in food, all vitamin K, whether K1 or K2, is partially or fully broken down in the body to K3, which is then converted to K2. It is therefore a transitional form not used in food products. Yet, as it is particularly effective in increasing the body's vitamin K2 levels and is inexpensive, it is used in megadoses in the diets of industrially reared animals, and in normal doses in other diets such as dog food. The vitamin K2 content of meat and liver can be high in meat products, particularly in processed meat products, because of the mega-dose of K3 in their diet. Extremely high doses of K3 worsen the antioxidant status and for this reason, it is not approved for use in supplements for humans, which is a pity because even small doses are very good at increasing the body's K2 levels.
Vitamin K1 has one type which is is phylloquinone, also known as phytomenadione.
Only one form of Vitamin K2 is found naturally in animals and humans in significant amounts, menaquinone-4 (MK-4). Very small amounts of longer-chain menaquinones can also be found in our liver, which are formed by intestinal bacteria mainly from vitamin K1 and stored in the liver to ensure that blood clotting factors can function for weeks in the event of vitamin K deficiency (e.g. starvation) so that we do not suffer stroke or embolism from fasting. In addition, fermented foods also contain these long-chain menaquinones (LC-MK), such as menaquinone-7 (MK-7). Various bacteria also produce all lengths between MK-5 and MK-14, conceivably MK-1/2/3 and menaquinone above MK-14, too. In dietary supplements, only MK-7 is still used in the EU, while in the USA the other forms are used, but only MK-7 and MK-4 are typical.
In the following, I will often use the terms MK4, MK7, and LC-MK to distinguish between K2s. By LC-MK I mean long-chain menaquinones, including MK-7 and all of them from MK-5 upwards. Typically, however, those between MK-8 and MK-12 are the dominant LC-MK in any food (cheeses, fermented plants) and in our guts.
Nutritional sources of K2 vitamins
Only modern foods contain it in any substantial amount. Until a few hundred years ago, it was not found in any food in any significant quantity! Why would I utter such nonsense? Yes, I was very surprised, too, I would have the same reaction...
Cheeses: the oldest foods that had effective amounts of K2 were aged cheeses. Cheesemaking, or at the least the making of hard cheeses, is not yet 1000 years old as far as I know, but I haven't looked into the matter much. The cheeses with the highest K2 content are the ripened cheeses, some of which can have as much as 100 mcg (/100 g), but a K2 content around 20-40 mcg is more common. Half of this is MK-4, the other half LC-MK (mainly MK-9 typically). Cheese was also the first food to contain LC-MK. This is significant because MK-4 is not even absorbed until it reaches multiples of 10 mcg (below 600 mcg there is no effect based on any study so far and no increase in blood or tissue levels at a lifetime dose, see later), but the utilization of LC-MKs is excellent and because of their slow half-life + excellent bioaccumulation, 100 mcg of them has quite a significant effect, which can be obtained from cheese. For this reason, cheese was the first source of K2 that contained effective amounts of K2, as LC-MK is effective even in small amounts, but should not be overdosed (see later).
Natto: Also a few hundred years old, a traditional Japanese "pickle" that supposedly tastes/smells pretty bad (I haven't tried it yet). Soybeans are fermented with a bacterium called B. subtilis and it produces K2, but only LC-MKs, specifically almost exclusively MK-7. 1 serving of natto (approx. 15-30 g) can contain up to 200-400 mcg of K2 in MK-7 form, which means about 1200 mcg/100 g, not that anyone can eat that much... The Japanese average is about 50-60 mcg K2 per day, while the largest natto consumers reach an average daily K2 intake of 160-180 mcg. Natto is not eaten daily.
Meats, offal: As I mentioned above, vitamin K3 is by far the cheapest of the K vitamins, while it also raises tissue K2 levels the most /mg (about 2-5x better than other K vitamins).(1)
That sounds good, but in fact, it is not so good for the tissues to use K2 exclusively and have no K1. K3 however cannot be converted to K1, only K2. Because K3 is much cheaper than K1, it is used to fortify animal feed. However, as K3 is less efficient than K1 at activating blood clotting factors despite being very good at increasing K2 levels.(2)
you need much more K3 and that is probably why it is used in such high doses in industry: they use up to 100-1000x the required dose to reach the desired effect because it is almost free.(3)
To get an idea of the K3 dose for animals: in the EU for example, it is common practice to fortify feed with 1-8 mg K3/kg, but the sky is the limit.(4)
Recalculated for human needs, this is equivalent to consuming about 5-10 mg of K3 per day, which increases tissue K2 levels about as much as roughly 20-30 mg of K2 MK-4 per day (due to absorption + molar mass), and if you include the refeeding of feces, you will arrive at a higher figure yet. So on a human equivalent basis, about 20-50,000 mcg of vitamin K3 equivalent to the intake of K2 is fed to animals on average, but e.g. in a study where unusually high levels of K2 were found in beef liver, cattle, and other industrially reared animals were given 100-800 mg/kg K3 (they were fed these levels not on account of the study, but as a part of their normal nutrition).(5)
I won't even calculate how much K2 would be in a human, but it's in the millions... In the US, the K3 dose in feed and formula is similarly high.(6)
Also, grazing animals are often given megadoses of K3 in their drinking water, even though the grass they graze is K1-rich. Coumarin is a common compound in grasses that causes vitamin K deficiency, a high dose of K3 is meant to counteract this.
As a result, animals fed this way can develop extremely high levels of K2 compared to those fed naturally. In industrially reared animals, high doses of K3 are commonly used, as it makes a poorer diet sufficient. In addition, in small or densely housed animals, it is also common to refeed one's own or another animal's feces. What does this have to do with any of it? It is because a significant proportion of the megadose K3 applied in such excess is not absorbed, but rather passes on to the large intestine and, as will be discussed, and is converted there by the gut bacteria into K2 (LC-MK). Their feces, therefore, contain most of the ingested K3, in the form of the K2 it is converted to. Their stool is a K2 (LC-MK) bomb, which when ingested, provides a gigantic amount of K2, more than the MK-4 they have converted from K3. We know from mouse/rat studies that LC-MKs are prone to proportionally displace MK-4 from tissues, especially the liver because they have a much longer half-life and better bioaccumulation, so after refeeding K2-rich feces in animals fed with K3, one would expect high LC-MK in their meat/their stool (especially MK-9/10/11, as these are the predominant ones in feces) and proportionally less MK-4. If the animal does not eat feces, the K3-rich diet will increase MK-4 levels. Looking through all the studies to date where K2 content of any meat/fish/offal has been tested, we find that any free range, non-K3 fed, but normally fed (grass grazing) animals have near zero K2 levels in their meat, liver and any organ/parts tested, typically around 2-4 mcg K2 MK-4 per 100 g. However, extremely high K2 contents have been measured in industrially farmed K3-fed animals, especially in processed meat products:
-
In foie gras pâté, 369 mcg/100 g of K2 MK-4 were once measured. LC-MKs were also measured, but there were none. Geese for liver pâté are fed with maize or other high starch, low K1 feed, which is therefore fortified with K3... I suppose a stuffed goose doesn't eat its feces, it's happy to have any room in its stomach, consequently, LC-MK levels don't increase, only MK-4 levels increase in both liver and meat (which was also measured and was 31 mcg/100 g, which is surprisingly high as well. Incidentally, 60 mcg have been measured in industrial chicken thighs).(7,8)
-
Although only 1-5 mcg K2 (/100 g) was found in the meat of free-range cattle, as in other measurements, there was almost none in their meat and liver, in one study ~100 mcg K2 (/100 g) was measured in the liver of a cattle fed a "megadose" (100 mg/kg) of K3, which was even more extreme than the usual megadose, and of which LC-MKs typical for feces was the major contributor...(5,9,10)
-
In a 2016 study we can consider relatively recent in this field, US store-bought pork prices were chosen to represent average consumption patterns. They were measured for K2 MK-4 and LC-MKs longer than MK-8 and found that the K2 content of bratwursts, sausages, and similar processed industrial pork products was very high: samples ranged from 300-500 mcg per 100 g, with the majority of the samples consisting of fecal LC-MKs. Fresh pork cuts were also analyzed, with K2 levels ranging from 40-100 mcg /100 g (also mainly LC-MKs typical of feces). This does not contradict previous measurements, because in the past K2 levels were typically only measured between MK-4 and MK-9, ignoring the fecal/colon types (MK-10-14). And in K3-fed animals, surprisingly high levels of MK-4s have been found in past studies already, as the fecal-type LC-MKs have only been measured in these industrially reared pigs.(11)
Interestingly, when measuring the K2 content of different meat cuts from free-range cows, they found that it correlated with lean meat cuts, i.e. the muscle cells contained the K2 (MK-4) rather than the fat, whereas in industrial pigs it correlated with fat, i.e. the fattier the more K2 (LC-MK). This is also logical, as there is a lot of LC-MK recovered through fecal refeeding, which accumulates due to its long half-life. As cells do not need so much K2, in fact, try to get rid of it, it accumulates in adipose tissue and correlates with it. However, the fat cells themselves do not need K2, so in animals not fed K3, which are reared with a natural, non-exaggerated intake of vitamin K, vitamin K2 is not in surplus. It is used up by the cells and therefore does not accumulate in fat, correlating with muscle tissue (protein) and not fat. Presumably, excess MK-4 can also accumulate in and consequently correlate with fat, not protein, but this has not been analyzed separately.
I will note, that it is hypothesized that high LC-MK concentrations in the gut enhance the otherwise very low efficiency of their absorption from the gut into the bloodstream, which would provide a more palatable but unlikely explanation for the high LC-MK content of industrial pork products. Since the LC-MKs formed in the gut are bound to the cell membranes of the bacteria that produce them and are not free for absorption, and the large intestine lacks the bile that is also required for K2 absorption, the possibility of such high levels of reabsorption is not excluded but is hard to fathom as an explanation.(12)
In any case, K2 has not been detected in the meat of wild animals (deer, rabbits) or the wild salmon of the Inuit, for example, nor even in the livers of seals (1-5 mcg/100 g), nor has it been detected in the various cuts of cattle grazing free-range grass. K2 levels in the meat/liver of animals without extreme doses of K3 nutrition appear to be negligible.(7,9,13)
So there is no reason to assume that we could have had access to any K2 other than MK-4 1000 years ago, and of MK-4, we should have been lucky to ingest 10-20 mcg. We can assume that the brain might have a slightly higher K2 content, but it is inconceivable that we could get even 100 mcg, whereas MK-4 doesn't even reach 600 mcg (see also later...) In other words, we can say that unless we used to eat feces regularly, we didn't get any significant vitamin K2, while industrial meat products are nowadays rich in K2. (I might add that the Hadza sometimes make a soup where they cook starchy tubers and spices with animal feces and then consume the juice. Supposedly it tastes even worse than natto...:))
Moreover, in awareness of the high K2 content of industrial meat, we can say that all the findings of epidemiological studies on K2 can be discarded, since only natto and cheese were considered K2-rich, and all other K2 content was presumed to be close to 0. However, if you are a fan of pork products consume the store-bought variety rather than the home-grown version, you have a good chance of getting 1-2 thousand mcg of K2 per day, and from a slow half-life, highly utilizable variety at that, i.e. the same or similar varieties as in cheese and natto (LC-MK). But the MK-4 content of 60 mcg per 100 g of chicken leg on feed is remarkable, too... In other words, high and low consumption of K2 were falsely assigned, so all data should be recalculated, merely the Japanese data might be correct, unless they were particularly strong consumers of pork in addition to natto -> all K2 epidemiological studies should be trashed until recalculated.
By the way, it sounds great that there is so much highly utilizable K2 in likely most of the processed meats, but as I will point out later, this can be a problem, because at high doses, K1 alone won't upset the ideal ratio in our tissues/organs, while such high doses of LC-MKs can presumably do so (360 mcg has already been shown to be counterproductive in a recent RCT study, but more on that later). It is easy to eat half a kg of sausages/salami/spare ribs a day, which can yield as much as 2000 mcg K2 (LC-MK), while 10 dkg of aged cheese is not consumed in a day even by gourmets, i.e. the consumption stays below 100 mcg, just as Japanese natto lovers stay below 200 mcg. We will see that LC-MK (or more precisely MK-7) has been found to be effective at amounts between 100-180 mcg, while higher doses are less effective or even counterproductive...
We will also see that in both humans and animals, the majority of vitamin K is in the form of MK-4 in tissues, even if only K1 is taken in and no K2. And it is now clear that our K2 intake must have been marginal. This means that vitamin K1 should be able to be converted to K2 at a sufficient level, i.e. our source of K2 was K1 during our evolution and should be today. So let's look at how much K1 is in food, and how much there must have been in the past...
Nutritioal Sources of K
Its richest sources are vegetables, some of which exceed 1000 mcg/100 g, but a more likely content is 50-500 mcg/100 g, although some are between 10,000-100,000 mcg/100 g m... Seeds and of course oils are also relatively rich in K1. While only 50-250 mcg/100 g are typical, these are much better absorbed than vegetables. Animal foods also contain a little. In the diets of native peoples that have been studied and our ancestors, vitamin K1 must have averaged 1000 mcg (1 mg) per day even when calculated with the vitamin K content of today's overbred vegetables/seeds which contain a fraction of the vitamins they used to, according to Cordain and Eaton.(14)
Presumably, it could have been as high as 5,000 mcg (5mg) if we assume that in less than 100 years the vitamin C content of apples has decreased by about a tenth to a hundredth... In contrast, today's recommendation is to consume about 100 mcg (0.1 mg) of K1 per day and that's about what people get, which is just enough to activate blood clotting factors. According to the aquatic-ape theory, the consumption of shellfish, crustaceans, seaweed, algae, and the like has played a crucial role in human evolution. Such marine 'vegetables' are extremely high in vitamin K1, containing up to nearly 1 million mcg K1 (/kg). Examples of algae commonly consumed today include wakame, nori, hijiki, and yendo (Sargassum muticum). 100g of these typically contain over 10,000 mcg K1, while yendo can contain up to 100,000!(15)
Could our ocean foraging ancestors have had access to enough K1 to produce sufficient K2? Shellfish (e.g. giant clams) often live in symbiosis with algae and shellfish played an essential role in our diet during our evolutionary phase near the East African ocean coast. So alongside the meaty "main dish" there was a super-rich "vegetable side plate" of K1... In addition, the transformation of K1->K2 is stimulated by zinc, magnesium, and D3 (see later). Wild animal meat and seafood (mollusks/shellfish) and K1-rich vegetables are all rich sources of magnesium, while all, with the exception of the latter, are also rich sources of zinc. The sun shone enough (D3). So our ancestors had everything they needed for abundant K2 synthesis, as do today's natural peoples: K1, D3, Mg, Zn.
We should not despair, even if we don't have such super K1-rich algae/seafood, 1 cup of cabbage cooked or as a casserole, cooked spinach or cooked beetroot, as well as chopped green salad contain about 500-1000 mcg K1 (/100 g), so if you like e.g. cabbage casserole or beetroot as a pickle, you should have access to around 1000 mcg of K1. (Heat treatment and fat increase the utilization of K1 from vegetables severalfold, so cabbage and kale stews, for example, are a great source of K1, providing up to over 1000 mcg of K1 per serving, in a form that is quite well absorbed).
In any case, there were plenty of sources of K1, while for K2 there was presumably only feces... In today's modern diet, our intake of vitamin K1 has been reduced to a generous tenth of that of primitive peoples, while if we take into account the excellent algae we eat today, it may have been reduced to one-thousandth that of our ancestors. In contrast, our vitamin K2 intake has increased significantly because of cheese, and in Japan because of natto, but especially in the last 50-100 years, since we have been eating K3-enriched foods, our direct K2 intake has increased by a factor of 100, which is not so good, as we shall see...
The distribution of the various types of Vitamin K in human and animal tissue
Human and animal organisms contain the highest proportion of MK-4 (typically over 70%), while the remainder is in the form of K1.(16)
Exceptions are the liver, which stores a small amount of K2 (LC-MK) produced by intestinal bacteria in some species, and also when the intake of LC-MK is unreasonably high, in which case it can no longer be converted to MK-4 in tissues-> it accumulates and upsets the natural MK4/K1 balance in tissues, although it is likely that such a quantity is only possible by refeeding of extremely high K2 (LC-MK) feces due to extreme K2/K3 intake (as in industrial pigs) or by direct administration of extreme doses of LC-MK.(17)
Small doses of LC-MK are transformed into MK-4 in the tissues without residue.(18,19)
Under natural conditions, therefore, only or almost only MK4 and K1 occur in animal/human tissues. This is true even if there is no K2 intake, only K1 intake. On the other hand, if there is no K1 intake, there will be no K1 in the tissues, which again poses a problem, but this cannot occur in nature even in obligate predators, since the prey animal's tissues already have K1 (typically 2:1 MK4/K1 ratio) + the plant food in their stomachs/intestines has a lot of K1, which is also consumed by predators.
Different tissues have different MK4/K1 ratios. For example, in brain tissue, kidneys, arteries, and testes, MK-4 is dominant, while in bones, heart, and liver, K1 is dominant.
In natural conditions, therefore, most of the vitamin K present in humans/animals is MK-4, while natural foods contain virtually no MK-4 (certainly not an absorbable amount), but more vitamin K1. And strangely enough, vitamin K1 supplementation increases tissue MK-4 levels as much, or in many tissues much more, than K3 or MK-4 itself! How is this possible?(1,20)
The absorption, metabolism, and transformation of K vitamins
Part of the vitamin K we consume is absorbed through our small intestine into our bloodstream and lymphatic circulation, while the unabsorbed part continues to pass through our intestines... How much of which form of vitamin K is absorbed and what happens to the unabsorbed part that has passed on in the intestine will be discussed later... Let's just stick to the part that is absorbed from the small intestine into the bloodstream:
Whatever vitamin K we ingest, be it K1, MK-4, or LC-MK, a significant proportion of it is converted to K3 in the intestinal cells (without relying on bacteria) and a small proportion is converted to MK-4. The K3 is then transported by the blood and lymph to our tissues, where it is converted to MK4 by the enzyme UBIAD1. What is not converted to K3 at the time of absorption, is mostly transported to the liver, where it is converted to MK-4 and exported to other tissues, already in the form of MK-4. And what is not converted to K3 in the intestinal cells at the time of absorption, nor to MK-4 in the liver, is transported to the tissues in its unchanged form and incorporated. In the case of K1, this is desirable, as all tissues/cells require K1, and many of our tissues prefer K1 over K2 (e.g. heart, liver, bones.) In the case of LC-MKs, however, they must be fully converted to MK-4, since they cannot be converted to K1 and have no function in LC-MK form. LC-MK at a viable dose can be fully converted to MK-4 in tissues, but not at excessive doses and there are several indications that this may be a problem, but more on this later. The point is that the LC-MK and K1 that are still in the tissues can be converted to MK-4 later because the enzyme UBIAD1 in the tissues excels at converting K3->MK-4, but it manages to convert other K vitamins to K3 as well, if more slowly. But the K stored in the tissues is not going anywhere, so there is time enough to do so.
Unabsorbed vitamins K that have reached the more bacteria-rich parts of the gut (end of small intestine + colon) are also converted to K3 by the gut bacteria but are then converted to LC-MKs rather than MK-4. It is questionable how much of these can then be reabsorbed back into the body. It is known that in the intestinal tract, nearly 100% of vitamin K1 is converted to K2 (LC-MK) in humans and that in the case of vitamin K1-deficient diets, none of the LC-MK produced by the intestinal bacteria is reabsorbed into the bloodstream, which is not surprising since it is first absorbed by the liver, which uses it to activate blood clotting factors, as this is the evolutionary preference (Triage theory). High vitamin K intake can lead to a high enough concentration of K2 in the gut, which also favors absorption + the liver doesn't use it all up, so it continues toward the tissues in the blood... This has never been investigated in humans, nor animals, but it is known that high levels of MK-9/10/11 have been detected in the meat of pigs and the livers of cattle raised on mega-dose K3 diets. It is still unclear whether this is due to increased intestinal absorption due to high LC-MK concentrations in the gut or rather due to the mega-dose of K3, which causes the LC-MK content of their feces to become very high, and the feces is then eaten by the pigs (let us not imagine that they are re-fed their feces on purpose, even though it is also known to be common practice... ). So it is not known to what extent the unabsorbed form of vitamin K in humans, converted to K2 by the gut bacteria, contributes to our K2 intake, but it likely contributes at least a little if vitamin K intake is high. In any case, even with low intakes of vitamin K, a small fraction of the LC-MKs produced in the gut reaches the liver where it is stored in case of starvation or vitamin K deficiency, because LC-MKs, unlike other K vitamins, have a very long half-life, so they can activate the blood clotting factors needed to stay alive for weeks or longer, which other K vitamins would be capable of for a few days only.
In summary, these 4 pathways of K1->K2 conversion are known:
1: During absorption, it is converted to K3 (and to a small extent to MK-4) in the intestinal wall, and the converted K3 travels via the bloodstream to the tissues where it is converted to MK-4.(21)
2: Incorporated into tissues, K1 is later transformed into K3 and then MK-4.(22,23,24)
3: In the liver, K1 is converted to MK-4, and is transported farther to other tissues such as the kidneys.(25,26)
4: Most of the unabsorbed K1 is excreted through the intestines, so it's bacteria in the small intestine + colon that convert it into K2 (LC-MK), some of which may be returned to our tissues through the liver and into the bloodstream.(12)
Of the 4 known modes, the first is considered to be the most important, i.e. K3 converted from vitamin K by intestinal cells during absorption is thought to be the main source of K2 (MK4) in tissues.
Let us nonetheless look at the preclinical and human clinical studies on the topic to see how efficient the conversion can be.
Comparative studies in animals on the effect of K1 and K2 on increasing K vitamin levels in the tissues
Of course, studies that investigate proportional changes in tissues following administration of different doses and types of vitamin K exist only in animals, as humans cannot be sliced up for study...
We know that poultry convert K1 to MK-4 faster/more efficiently than pigeons. We also know that rodents are even less efficient than pigeons. In comparison, studies on mice/rats also show that they convert K1, if not quickly, then still with perfect efficiency, even at extreme doses, and while K2 shifts the natural tissue ratio, K1 does not and is converted to K2 indefinitely while preserving the natural tissue ratios!
Studies:
In one study, they looked at how the vitamin K content and ratio in the organs/tissues of rats changed when they were given different vitamin K intakes for 16 weeks. One group was given a vitamin K-free diet, another group was given a vitamin K1-rich diet, a third group was given a vitamin MK-4-rich diet, a fourth group was given a vitamin MK-7-rich diet and a fifth group was given a vitamin K3-rich diet. The K1-rich diet alone did not overwhelm the natural MK4/K1 ratio of the tissues, while it was just as effective at increasing tissue K2 levels as K2, and in some tissues, it increased K2 MK4 levels significantly more than MK4 itself! Such tissues included the brain, testes, and bone, among others. MK-7 was detected only in the liver, kidneys, and bone, and of course only in the group receiving MK-7 (the amount was unviably high -> presumably it could not be fully converted). K3 was the most effective in increasing tissue K2 levels, although it was only given at half to one-third the dose of the others (in mcg, because of its lower molecular weight), i.e. a vitamin K3-rich diet is 2-3 times more effective in increasing tissue K2 levels (as we have seen in the meat of animals fed megadoses of K3).(1)
As I mentioned, K1 was also better than MK-4 itself at increasing brain K2 (MK4) levels. Raising MK-4 levels in the brain is quite tricky because only K3 can get through the blood-brain barrier to any significant extent, as it is much smaller than the other K vitamins. So K vitamins must first be converted to K3. Not surprisingly, yet another mouse experiment found K1 to increase MK-4 levels in the brain more strongly than vitamin K3.(20)
In one study in mice, a human equivalent of about 90 mcg of MK-7 was administered and the mice bone tissue was examined for its effect: MK-4 levels were increased, while MK-7 was undetectable, i.e. completely transformed.(27)
In another study, it was also found that MK-7 acted by conversion to MK-4 in the body.(19)
In two different studies, it was no longer able to fully convert to MK-4, thus upsetting the tissue MK-4/K1 ratio.(1, 28)
It's unclear how much of a problem this is, but in one of the two studies the effects on skeletal health were also examined, and high-dose K1 had a good effect on skeletal health, while both high-dose MK4 and high-dose MK-7 worsened several indicators of skeletal health. This may have been caused by an upset in tissue ratio, i.e. that they proportionally displaced K1. High-dose MK-7 had the worst effect. It would therefore seem that the K1 form has the most significant effect on the skeleton, and it is no coincidence that it is the dominant form in bones. Presumably, tissues/ cells can adjust their ideal MK4/K1 ratio by simply changing the release of the UBIAD1 enzyme, i.e. if more K1 is ideal for a tissue, it releases less UBIAD1 -> less K3, and in consequence, less MK-4 is formed from the already incorporated K1, leaving it in the form of K1. This is a good strategy as long as no excessive doses of LC-MK are applied because then it's not K1 that remains in the tissue, but LC-MK, which has no business being there.
In another study, mice were pretreated with warfarin to induce coronary atherosclerosis and then given high doses (about 50 mg/day in humans) of K1 or MK-4 for 6 weeks. Both treatments reversed, with MK-4 reducing the size of the calcified plaques by about half within the treatment period, while the K1 treatment was even more effective, reducing their size to nearly a third! When the coronary artery wall was examined, it was found that both treatments increased MK-4 levels in the tissue by about the same amount (many times more than in control mice). However, while MK-4 administration completely displaced K1, upsetting the natural vitamin K ratio (MK4/K1) of the tissue, the more effective treatment, K1 administration, achieved the same MK-4 increase while maintaining the natural tissue ratio.(29)
It is important to note here that in a previous mouse experiment, warfarin was given simultaneously with K1 and K2, and thus K1 did not prevent calcification, while K2 did. This demonstrated that K1 must be converted to K2 to have an effect in preventing atherosclerosis.(30)
We will see that K1 has also been shown to be the most effective in humans in completely stopping atherosclerosis, even at a dose as low as 1 mg, while MK-4 cannot achieve the same even at a dose of 45 mg. Since we know that to be effective in stopping atherosclerosis, K1 needs to be able to convert to MK-4, it is not really a question of how much K1 can convert to K2 in humans: Exactly as much as needed is converted. Perhaps that's why K1 has performed better than K2 in many studies, because it increases K2 levels to precisely the necessary level and not beyond... K1 increases K2 levels while maintaining the natural tissue ratio, whereas K2 easily shifts the natural tissue ratio.
I have not looked for studies in other animals, given that the most common vitamin K supplementation for all animals is to fortify their diet with K3. It is the same in dogs, cats, but also in cattle, pigs, rabbits, birds, and the rest, so it follows that all animals, even predators, can convert K vitamins to K2 efficiently by themselves, otherwise K3 would not be effective and they would not administer it...(3)
Conversion in humans
In humans, 2 studies have looked directly at conversion. In one, blood was tested only 6 h after a single 40 mg dose of K1 and only to see whether the K1->K3->MK-4 conversion follows the same pattern in humans as in mice. They found that indeed, K1 conversion occurs in the same way, following the same pattern, with apparently the same efficiency in humans as in mice.(21)
In a previous study in 2006, subjects were given 10 mg K1, 15 mg MK-4, or 1 mg MK-7, and their urine was collected for 24 hours. The amount of K3 excreted in the urine was used to infer how much K1 or MK-4 or MK-7 was converted to K3 and then MK-4 in the body...(31)
It has been found that in 24 hours, 5-25% of the ingested (and unabsorbed!) dose is converted to K3 (which is then converted to MK-4 in tissues) with K1 conversion ranging from 8-30% for the ingested (not absorbed) dose. This study, however, measured only the conversion during absorption (the other three modes of conversion mentioned above were only revealed in studies years later). The study reported the route of administration of the doses, which allows the rate of absorption to be calculated, i.e. about 50% of the K1 absorbed into the bloodstream was converted since the absorption from the blood was between 20-50% for the route used. So in the first round, up to 50% of the absorbed vitamin K may be converted to K3, then MK-4, and later more in the tissues. I should add that a 10 mg dose was studied, and the conversion processes, as well as the utilization, are generally characterized by a less-is-more logic, i.e. if a smaller, more viable dose of 1-2 mg had been taken at a time, a better conversion rate may have been reached. However, even on these grounds, the K1->K2 conversion in humans is still working fine. You will see that this is supported by how effective vitamin K1 is in most of the placebo controls and any human studies performed so far. I also found another human study...(32)
...where they didn't examine at this, but you can infer from it nonetheless: 4 days after delivery, they gave pregnant women 2-4 mg of K1, well absorbed, but as a tea, not with food, so this 2-4 mg dose is equivalent to about 1-2 mg in meal form, dissolved in oil. It was administered for 12 days only. In the meantime, those receiving the lower dose had a significant increase in their milk, while the mothers receiving the higher dose also started to have a significant increase in their blood levels of MK-4 (which more than doubled), which is surprising. If Chris Masterjohn's theory holds true, that MK-4 is only utilized past an ingestion of 600 mcg, because at lower concentration it is immediately taken up by the tissues from the bloodstream, then that means that the nutritionally viable dosage intake of K1 for 12 days was able to fully replenish the MK-4 levels in the bodies of the postpartum mothers, despite also excreting MK-4 and K1 in their milk, because if there is excess MK-4 in the blood, it must mean that the tissues/cells are saturated. By the way, this theory of Masterjohn's is contradicted by a study where a low dose of MK-4 was not able to increase tissue MK-4 levels by any amount.(19)
In any case, vitamin K1 taken for 12 days increased the MK-4 levels of the pregnant women to a similar extent as MK-4 levels in the Japanese subjects of a study, who had taken 1500 mcg MK-4 per day for six months, while also consuming a significant amount of natto, which was not documented in the study, but is clear from their high blood levels of MK-7 and the fact that the subjects were Japanese.(33)
I could only find a single study where MK-4 levels were measured in people taking MK-7, but no MK-4 whatsoever was detected in their blood at any time. However, the dose was only 100 mcg per day, and only for about 100 days. Of course, it could have increased in their tissues regardless of blood levels. The blood levels don't matter much, they just show that they are saturated.(34)
The effectiveness of the conversion depends heavily on certain micronutrients and medicines:(25,26,35,36)
Vitamin D3 enhances the conversion of K1 to K2 in the liver and kidneys, while vitamin A (retinol) is needed to transport K1 to other tissues and/or to enable K2 to activate the corresponding proteins (MGP). Vitamin B6 also aids in activation. Zinc increases the expression (production) of the enzyme UBIAD1 responsible for conversion in our tissues, while magnesium increases the function/efficiency of the same enzyme to form more MK-4. In addition, retinol itself is great at activating MGP, although this may just be due to its effect of supporting vitamin K's function, but ultimately it makes no difference.
Conversely, the following drugs inhibit the conversion of K1 and LC-MK to MK-4: cholesterol-lowering statins, bone-strengthening bisphosphonate drugs, and stone-age anticoagulant drugs (vitamin K antagonists such as warfarin). If you are taking these drugs, you may want to take MK-4 (unless you are taking Warfarin or similar coumarin derivatives, as these inhibit all forms of vitamin K, but it is better not to take them at all, there are more modern ones available that are unproblematic).
As for the efficiency of the conversion, I think it can be said that exactly as much K1 as needed is converted to K2 in the human (and animal) body in the tissues, and that is why K1 is the best because it can remain K1 if that is the preferred form for the tissue. K2 and K3 can't convert to K1, but K1 can and does convert to any of the forms, as long as we don't become D3/zinc/magnesium deficient and have to take the drugs listed.
On the absorption/utilization of K vitamins
We have seen that whatever vitamin K we consume is eventually converted to MK-4 (except in tissues that are also happy with or prefer K1). So, in terms of tissue levels of vitamin K, they are actually all equally good (the ratio can only be shifted by high doses). So, the degree to which a unit amount of them will improve our vitamin K levels depends mainly on their absorption/utilization. This is based on two factors: how much of the amount consumed is absorbed into the bloodstream (absorption) and how quickly it is excreted from the body, or at least from the blood, as this is the only thing that can be measured, called the half-life.
The absorption of vitamin K1 from raw vegetables is typically quite poor, between 3-10%, while it is around 25% when cooked and/or in fat, and even higher for some vegetables. Vitamin K1 dissolved in oil with a meal containing sufficient fat has an absorption of around 80%. Most of the unabsorbed amount is converted by bacteria in the intestine into K2, although little of this is reabsorbed. The absorbed portion of K1 is rapidly metabolized, with a half-life in the blood of about 6-7 hours (when consumed with a meal, as with vegetables, and only about 2 hours when consumed on an empty stomach as a supplement). Only amounts beyond this reach other tissues. The portion that does reach tissues is converted to MK-4 in the proportion appropriate to the tissues.
K2 MK-7 achieves 80% utilization from any source, and fat is not important for proper absorption. So about 80% of the intake reaches our tissues. The tissues, however, are very slow to absorb it (maybe because it's not required?), so it circulates in the blood for a very long time. Its half-life is long and consists of two phases of disintegration: like K1, its primary half-life is 6-7 hours, but then its half-life slows down and takes another 2-3 days to halve. Once it reaches the tissues, they convert it to MK-4, as they do K1. Because of its slow half-life and excellent absorption, it has about 3 times better utilization than K1. I calculated this from a study comparing the same dose of K1 and MK-7, which found that MK-7 bioaccumulates at a rate 6-7x higher than K1, while its delivery to bone is 3x better than K1. It is even up to 5x better at activating blood clotting factors. However, the study used a dry, undissolved form, which has an absorption of about half to one-third of that of a normal, dissolved form of vitamin K1 taken with food, while the absorption of MK-7 is excellent in this form as well. With this in mind, the above figures should be halved at least, i.e. 2-3x more effective with the same amount of MK-7. Then again it is 100x more expensive and can easily be overdosed precisely because of the slow half-life and because it can shift tissue ratios.(37)
The utilization of MK-4 is an interesting question because from the current human clinical trials we know only that up to 500 mcg of it was not able to show up in the bloodstream at all. Nor do we know whether this is because it is so poorly utilized or because the first blood sample was taken 2 hours after ingestion and by then it had all been taken up by the tissues and disappeared from the bloodstream (this is Masterjohn's theory). This is unlikely, as mouse experiments confirm that low dose MK-4 failed to increase tissue MK-4 levels, while MK-7 was able to increase both blood and tissue levels.(1)
Another explanation is that the ingested MK-4 is completely converted to K3 during absorption in the intestinal cells and therefore does not appear in the bloodstream as K2, but this is also unlikely because of the previous study, which should have increased tissue MK-4. Finally, it is also possible and seems most likely, that it is simply not absorbed up to 500 mcg. This is suggested by another human study, where MK-4 was given to healthy people at a higher dosage each week to determine when it starts to activate osteocalcin, i.e. when it starts to have any effect. In the first week, 300 mcg MK-4 per day caused no change. By the end of the second week, 600 mcg a day had started to show an effect, but real effects started only above 900 mcg. This confirms studies that found that doses of 420-500 mcg had not yet appeared in the blood -> not enough of it was absorbed to reach the detection limit -> not enough was utilized. However, it cannot be ruled out that in the long term, MK-4 below 500 mcg could be effective, it is just that the current evidence makes it very uncertain. Be that as it may, the threshold dose is around 600 mcg.(38,39,40)
The best study on the efficiency of the utilization of different K vitamins in humans was done in 2002, where equal amounts of K1 (about 900 mcg), K2 MK-4 (about 1000 mcg), and LC-MK (MK-9) were dissolved in butter (per person) in equal molar (molecule per unit) amounts. This was given to the participants with breakfast, and their blood was periodically drawn and the amounts in their blood were monitored. K1 resulted in the highest blood peak and also, at first glance, the best utilization, but the long half-life of MK-9 makes it difficult to know which was better overall. In any case, it is clear that the recovery of K2 MK-4 was about a third of that of K1 (calculated from the area under the curve, AUC). In addition, the half-life of MK-4 was 4.5 hours, while that of K1 and MK-9 was 6.5 hours, but after MK-9's level dropped to a quarter, it was only 2 days later that it dropped to half, i.e. it had a double half-life, just like MK-7, as was to be expected.(41)
Overall, therefore, LC-MK (e.g. MK-7) seems to be the best utilized, vitamin K1 is also good, while MK-4 is poorly utilized and presumably only at supraphysiological doses. Considering what we have found, namely that MK-7 has 3x better utilization than K1, which is 3x better than MK-4, this is what follows: 200 mcg K2 MK-7 has an effect equal to 600 mcg K1, which is equal to 1800 mcg K2 MK-4. And that's pretty much in line with what we'll see in human studies: MK-7 is most effective between 100-200 mcg, K1 starts to be effective above 500 mcg, and MK-4 above 1500 mcg.
The functions of Vitamin K in the body
The main function of vitamin K is to activate vitamin K-dependent proteins.(42,43,44,45,46,47,48) There are a few of these, but 3 are the most common:
-
Activation of blood clotting factors: 100% activation of these is important for regulating blood clotting (they help blood clotting but also inhibit excessive blood clotting, so they cannot be overdosed and they cannot "thicken" the blood as many people believe). K1 and MK-7 are excellent at activating these factors, MK-4 less so.
-
Activation of osteocalcin (ucOC): this is mainly found in bone and the dentin layer of teeth, and its activation is most indicative of the effect of any particular vitamin K on bone/teeth but is also associated with insulin sensitivity and other factors. In humans, studies to date have shown that K1 is by far the most activated: as little as 500 mcg per day activate fully, but it is maximal at 1000 mcg. MK-7 is also activated at doses of 100-200 mcg per day, and MK-4 above 600 mcg per day.
- Activation of Matrix-Gla proteins (uc-dpMGP): these are also found in the skin, joints, and dentin layer of teeth, but mainly in the walls of arteries and veins. How well a type of vitamin K can activate it shows how well it can prevent and reverse the calcification of blood vessels. Again, K1 is by far the best at this in humans (500 mcg of K1 per day can activate it almost completely). MK-7 can also activate it, but less well efficiently, while MK-4 has never been measured in humans.
However, MK-4 also has effects that it alone can do: it modifies gene expression, which can induce hormone production, and much more. MK-4 is the most important in the body, so it's no wonder that all vitamin K is eventually converted to MK-4 in humans and animals alike (except for K1, which is not converted by the tissue because it needs it in the form of K1, not MK-4.)
In addition, presumably, MK-4 is also required for activation of uc-dpMGP. This is at least what a study suggests wherein the inhibitory effect of K1 on atherosclerosis was eliminated by inhibiting K1->MK-4 conversion with warfarin, while MK-4 administration was still effective.(30)
In a study by the same researchers 4 years later, where they did not inhibit the K1->MK-4 transition with Warfarin while administering K1, it was also significantly more effective than the same dose of MK-4: pre-existing calcification was reduced by about 60% by K1 over 6 weeks, while MK-4 only reduced it by about 40%.(29)
In another mouse study, osteoporosis in mice was achieved by removing their ovaries (exaggerating and roughly mimicking post-menopausal osteoporosis). Measured in the human equivalent, one group of mice received about 50 mg of K1 per day, another group received about 65 mg of MK-4, and the third group received about 85 mg of MK-7, while the control group received nothing. K1 proved to be the most effective. The members of the K1 group also had a better bone density, bone strength, and bone mineral density than the control group, while the members of both the MK-4 and MK-7 groups performed worse than the controls, especially the MK-7 group. Thus, at high doses, only K1 proved to be mildly effective, while high doses of both types of K2 proved to be counterproductive.(17)
K1 is the dominant, if not the only, vitamin K naturally present in bones. High doses of MK-4 and MK-7 have upset the balance by their high incorporation into bone. And MK-7 has no place there, while the unchanged incorporation of MK-7 in the bone tissue of animals.(27)
MK-7 accumulation does not seem normal, it is understandable why it is the most destructive one compared to the control. Bone tissue was strongest if only K1 was incorporated into it, as is the norm. In other words, for the skeleton, K1 itself appears to be the most important form, untransformed.
So it seems that the MK-4 form is required by the body for the cardiovascular effect to be realized, because if the K1->MK-4 conversion is inhibited, there is no effect of K1, whereas if it is not inhibited, it is more effective. In addition, it appears K1 itself is responsible for the positive effect on the skeleton, it does not need to be converted to MK-4. Vitamin K1 is therefore the best vitamin for all vitamin K functions in the body, but only if the conversion to MK-4 is not inhibited by drugs, as only MK-4 can induce gene expression and presumably activate MGP protein.
It is also worth mentioning the role of MK-7 and other LC-MKs. They are produced by the intestinal bacteria, and almost all of the unabsorbed K1 is converted into these K2s, which are transported to the liver and stored there. In the event of vitamin K deficiency (e.g. starvation), they can keep blood clotting factors activated for weeks or longer, which is very important for survival. LC-MKs are needed for this because their half-life is not a mere 6-7 hours but can be as long as 1-2 weeks, i.e. they can prevent haematuria and clot formation for weeks in the case of starvation, whereas MK-4 and K1 would require daily intake. This may therefore be the evolutionary function of MK-7 and other LC-MKs. This is the reason we are in symbiosis with our gut bacteria, to send LC-MK to our liver, so we don't get embolism/stroke from a few days of vitamin K deficiency.
Resolving discrepancies
The illusion of the ineffectiveness of vitamin K1 is perpetuated by references to studies that are clearly irrelevant. These include in vitro studies, where it is natural that there is no effect since the K1->MK-4 conversion only takes place in living organisms. Then there is a study on mice, mentioned above, where K1 and K2, although at the same dose, were given huge doses of warfarin throughout the treatment, which completely inhibits the conversion of K1 to MK-4 and its effect, so it is no wonder that K1 did not prevent warfarin-induced calcification there, while MK-4 did.(30)
However, the study was repeated 4 years later, but in this case, they had previously induced severe calcification with warfarin and then suspended its administration, and so now vitamin K1 was not only simply effective but was significantly more effective than K2, reversing the existing calcification to a degree nearly one and a half times greater.(29)
Intervention studies have been cited, but these also used drugs that inhibited K1-MK-4 conversion to undermine the effect of K1 (I will deal with this later in the human studies). But the most common reference for the ineffectiveness of K1 and the effect of K2 is the famous Rotterdam study, which bleeds from many wounds. In fact, they quite ridiculously tried to shove down our throats that a 14 mcg difference in K2 between the two groups halved the mortality from atherosclerosis, and accounting for that dose solely by the consumption of cheese at that... Before I come to that, two sentences to help you understand the rest:
According to the "Triage theory",(49) up to about 50-100 mcg of absorbed K1 is used to activate blood clotting factors and nothing else, which is an evolutionary preference. Amounts exceeding this are only taken up by the bloodstream to other tissues (already converted to K2 in whole or in part). Since absorption efficiency from food is typically only around 20%, less than 400 mcg of K1 from food may not have much effect.
This is exactly what has been shown in epidemiological studies:
- In the much-cited 2004 Rotterdam study,(50) K1 and K2 dietary data were estimated from a single, non-repeated, weak questionnaire test, were analyzed separately (!) among Dutch residents, and found that those with the highest K2 intakes (average 41 mcg/day, mainly from ripened cheese) had a lower incidence of certain cardiovascular diseases and a 20-50% lower rate of mortality from causes related to those diseases than those with the lowest K2 intakes (27 mcg/day). That's only a 14 mcg K2 difference... a ridiculous assumption... Even in the highest K1 consuming group breakdown, the daily estimated K1 intake was only 337 mcg, of which 100 mcg absorption was just barely achievable, so it's no wonder that it only reduced cardiovascular risks/deaths by about 10-20%. Half of the 14 mcg K2 was MK-4, and the other half was mostly MK-9. For MK-4, obviously, a difference of 7 mcg makes no difference seeing as it is not even utilized up to 500 mcg. If it was a K2, then MK-9 could be just the cause of the reduced risk, but from 7 mcg? I'd rather guess that those who consume gourmet aged cheeses (since that's where the participants' K2 mainly came from) are typically not junk-food lovers... better food choices, etc...
A few similar epidemiological studies have been done, but they found much milder associations, all with very low K1 consumption, so it's not surprising that it was not found to be effective, although there were studies among them, which did show effectiveness.(51,52)
As if that wasn't enough, there is another argument in itself, which has already been mentioned: since 2016, we know that processed meat dishes often have extremely high K2 levels.(11)
Moreover, like cheeses, they contain mostly LC-MKs. In all epidemiological studies to date, the K2 content of meats has been taken to be close to zero, but 1 piece of sausage or bratwurst can contain up to 300 mcg of K2, as it turns out, even a small 10 dkg slice of ribs can contain around 100 mcg. In other words, someone who eats a lot of industrially raised, processed pork may well be getting up to 1000 mcg of K2 per day, about 20 times more than the highest category measured in the studies... So their measurement is completely off, cheese consumption is not representative of K2 intake, not even if we narrow it down to LC-MK, as K3-fed pork contains LC-MK as well, except in much, much higher amounts. It is hard to eat 100 mcg K2 a day from cheese, yet from industrial meat, even consuming 1000 mcg becomes easy. You would have to recalculate the whole thing so that processed industrial meat products are not calculated with a K2 value close to 0, but with say 50-100 mcg /100 g...
10 years after the publication of the Rotterdam study's K2 analysis, in 2014, the PERIMED study used a repeated questionnaire method, about 3 times more accurate than the previous ones, to assess the nutritional characteristics of about 7200 people with high cardiovascular risk factors who eat a Mediterranean diet. It is also the first study to assess K1 and K2 consumption and their relationship, i.e. the first serious epidemiological study on the subject (as far as an epidemiological study can be taken seriously), but the main reason it was interesting is because here the top K1 consuming group had an average daily intake of 626 mcg K1, of which surely more than 100 mcg is absorbed -> it gets past the liver to all tissues in abundance, in the form of K2 MK-4, or is converted to this form locally... This study also had a broader spectrum of K2 consumption than the previous ones, which also improves the comparison and accuracy of the study: 18 mcg was the lowest and 58 mcg the highest average daily K2 intake in the group analyses. Of course, the high K2 LC-MK content of industrial meats has not yet been accounted for here, so the findings for K2 in this study are also incorrect. The highest (average 626 mcg) K1 consumers had about a 50% (!) reduction in both cancer and cardiovascular mortality, including stroke, and even all-type mortality was reduced by 40%! In contrast, among the highest K2 consumers, there was no reduction in deaths, no effect, which is not surprising, since you wouldn't expect anything from 50 mcg K2, which is mostly MK-4 + they guessed wrong on K2 intake in the first place (industrial meats).(53)
Studies on the effects of the various types of Vitamin K, in interventional studies
So far, we have discussed the occurrence of vitamin K in food, the amount of vitamin K consumed during our evolution, its distribution, metabolism, transformation, and absorption in the body. Further, we have discussed indicators of their effects on the skeleton and cardiovascular system, i.e. their activating effects on osteocalcin and matrix Gla proteins. However, the actual clinical outcome, i.e. what graspable effect it had on improving conditions or reducing the risk of disease has at most been mentioned. I have also presented relevant epidemiological studies.
It can be seen that vitamin K1 is efficiently converted to K2 (in at least 4 ways, as mentioned above), whereas at high doses only K1 can increase MK-4 levels without overwhelming the corresponding ratio. At low doses (~100 mcg) it is used up in the liver to activate coagulation factors and is rapidly metabolized, but when consumed at normal levels (200 mcg+), or as has been typical of us throughout our evolution (>1000 mcg), it should be able to provide ideal levels of vitamin K2 and should be at least as good or better than K2 when consumed at nutritionally viable doses. Similarly, supraphysiological doses of K1 should be at least as good in humans as has been seen in animals. Of course, any theory can only be as good as practice proves it to be. The proof of the pudding is in the eating, so let's look at the normal placebo-controlled human clinical trials, RTCs, since the human trials mentioned so far had no clinical endpoints, epidemiological studies can only establish correlation, not causal relationships, and the animal studies were, of course, not done on humans... Does this all back up the fact that in normal placebo-controlled trials K1 performs at least as well as K2? (Spoiler: it does)
Before we get to that, however, I'll briefly describe below the intervention trials mentioned earlier once again, just to put them in the same place as the others.
Preclinical comparative studies
Since there are more than enough human clinical intervention studies, I looked for only those animal (pre-clinical) intervention studies that compared different forms of vitamin K. I found 2 such studies that also looked at physiological effects, not just tissue levels or indirect indicators, and where no drug was used to inhibit vitamin K conversion simultaneously with vitamin K administration. Both studies have been described above, so I will now just briefly outline them:
In one, a human equivalent dose of approximately 50 mg per day of K1 or K2 MK-4 (or nothing) was given to one group of mice each, after having previously induced severe calcification in their aortas and coronary arteries. In the group receiving vitamin K1, the size of calcified plaques was reduced to nearly a third after 6 weeks of K1 supplementation, and the elasticity of blood vessels improved greatly, too. K2 MK-4 was also effective, although less so, reducing the size of calcified plaques by "only" half. The levels and ratio of MK4/K1 in the aortic tissue were also examined. Taking both K1 and MK-4 increased aortic tissue K2 (MK4) levels by roughly the same amount, but while K1 did so while maintaining the original natural 2:1 - 3:1 MK4/K1 ratio, the ratio was disturbed in the group taking K2; K1 was displaced. This may be the reason for the poorer performance of high-dose K2 compared to high-dose K1.(29)
Another study simulated postmenopausal osteoporosis in mice by surgically removing their ovaries.(17)
One group of mice was given moderately high doses of K1, MK4, or MK7 and the effects on their bone structure were compared with a group that had been operated on but not given vitamin K. Those in the K1 groups improved their condition on all 3 parameters measured, while those in the K2 groups showed no improvement and even showed deterioration on 2 out of 3 parameters. The measured parameters were bone strength, mineral density, and elasticity. MK-7 had the worst effect. Surprisingly, therefore, only K1 proved to be somewhat effective, while the use of K2 vitamins was counterproductive, most notably in the case of MK-7. Tissue ratios were measured in bone and here again, it was found that K2, especially MK-7, upset tissue vitamin K ratios while K1 did not. So it seems that this ratio is important, and in the case of bone, the displacing K1 not only means diminishing the positive effect, as had been the case for the vascular system in the previous study but even bearing an outright negative effect.
Placebo-controlled human intervention trials of the activating effects of vitamin K on osteocalcin and MGP, i.e. blood-measurable indicators of vitamin K effects:
I have already presented this in the section on vitamin K functions, so now just 2 sentences about it:
Both osteocalcin and MGP are by far best activated by vitamin K1 (around 500-1000 mcg per day). The activating effect of MK-4 MGP has never been measured. It can therefore be said that vitamin K1 is the best in humans for the two most important effects attributed to vitamin K2 and that it realizes this effect in the amounts ingested with a perfectly normal, healthy diet.
Finally, for the most exciting part:
Placebo-controlled human trials with clinical endpoint
Human trials comparing K1 and K2 directly:
First, there are 2 direct comparisons, K1 vs MK-4 and K1 vs MK-7. Comparing studies of different designs to each other is obviously difficult and can easily be deceptive. A clear conclusion can only be made when they are tested in the same study, in the same design. Unfortunately, there are only 2 of these, which is not surprising, as they showed that K1 is better than K2, which is in nobody's financial interest... Let's see:
K1 vs K2 MK-4
In a 2009 US study, 389 post-menopausal women were given 400NE D3 + 630 mg Calcium citrate for 1 year. They were divided into 3 groups. One group also received 1mg (1x1mg) of K1 daily, another group received 45mg (3x15mg) of K2 MK-4 daily, while the third group received only a placebo with D3 and Ca. Apparently, in this case, D3 and Ca were enough to keep their bone density from deteriorating, but they also measured the change in ucOC levels. 1mg K1 per day was able to reduce uCOC by 62% over 1 year (from 13% to 5%), while 45mg per day was able to reduce uCOC by 60% (from 11.6% to 4.6%). Surprisingly, 1mg of K1 had the same effect and was even a shade better than 45 times as much K2 MK4. No wonder they chose not to study it further, especially since the study was commissioned by Eisai, the manufacturer of the K2 MK-4 drugs...(54)
K1 vs K2 MK-7
2011 study, 173 Greek participants aged 60-62 years received either 100 mcg K1 supplementation per day (110 mcg average dietary K1 intake) or 100 mcg K2 MK-7 per day (140 mcg average dietary K1 intake) for 1 year. Both groups also received 400NE of D3 + about 1000 mg of Ca + about 400 mg of Mg in their diets. There were also two placebo groups, one didn't receive any vitamin K, and the other didn't receive any D3, either. So the four groups were K1+D3+Ca+Mg / K2+D3+Ca+Mg / D3+Ca+Mg / Ca+Mg.
The group receiving K1 supplementation had a 1.6% increase in measured spinal (lumbar) bone mineral density (BMD) while preventing soft tissue calcification. The urinary marker of bone loss (D-Pyd) decreased by 22%.
K2 MK-7 also prevented soft tissue calcification and reduced urinary loss of a bone marker by 21%. However, it increased the measured spinal (lumbar) bone mineral density by only 0.6%, i.e. K1 supplementation improved the bone density of the spine almost 3 times more than the same dose of K2 MK-7, showing an equal effect in all other arenas.
Both vitamin K treatments significantly improved the ratio of inactivated to active osteocalcin, which was worsened in both placebo groups, as they did not prevent calcification and of course did not improve spine mineral density.
So in one case K1 performed better than the same dose of K2 MK7, while in the other case it performed identically to the 45x higher dose of K2 MK-4... Obviously, this was not what was expected in either study. The results are surprising and very useful, i.e. they should very much be investigated. 10-12 years have passed and no studies have been done since then, because the economy is doing so well, selling expensive K2 instead of K1... less effect, more money, everyone benefits but the patient.(55)
Placebo-controlled trials to determine the effect on bones
In a 2009 review, it was found that placebo-controlled trials published up to that time had already found vitamin K1 supplementation to be effective at a nutritionally viable level (0.5-5mg), whereas only supraphysiological/pharmacological doses of K2 were effective. Only 45mg of K2 (MK-4) has proven effective. A significant reduction in fracture risk or other similarly significant effects beyond the activation of osteocalcin started at a 5mg dose of K1 and a 45mg dose of K2, which reduced the fracture risk by about half. The 45mg dose of K2 reduced the relative fracture risk by 39-56% in the trials, while the 5mg dose of vitamin K1 reduced it by 55%! Osteocalcin activation was also similar.(56)
A 2017 meta-analysis found that vitamin K1 consumed with meals significantly reduced fracture risk.(57)
Placebo-controlled studies with K1 on bone mass
In 10 out of 10 RCTs, it was found to be effective in improving the ocUC/cUC ratio, i.e. activation=carboxylation of osteocalcin (an indicator of a positive effect on bone mass measured in the blood), while a direct effect, i.e. a positive effect on bone density (reduction in osteoporosis rate or increase in bone density) and/or reduction in fracture risk, was found in 5 out of 10 trials. However, if we exclude the irrelevant studies, we end up finding that K1 had a direct effect in 100% of the studies. Here are these 5 irrelevant studies out of 10 and why they don't matter:
- There was a 36% use of statin, which inhibits the conversion of K1->K2 + there was no improvement compared to the placebo group merely because there was no deterioration in the placebo group.(58)
- They were using a poorly absorbed form and little of it (500 mcg in effervescent tablet form of which only about 100 mcg can be absorbed), a fact that was even explicitly mentioned in the study. They were surprised that their blood levels of vitamin K1 barely increased compared to the dose, i.e. not absorbed due to poor administration.(59)
- This was a 6-week study. Of course, whatever the dose of K2, no change in the bone occurs within 6 weeks, only in the blood levels, which is what happened.(52)
- Once more, the reason why the bone density decrease did not stop compared to the placebo group was that there was no deterioration in the placebo group (45mg MK-4 was taken by the other group, which did not increase bone density either, 45mg K2 had the same effect as 1mg K1).(54)
- Hormone-disordered, over-worked young female athletes... it seems they are not helped by K, only by estrogen replacement or steroids and ceasing the excessive training...(60)
If we exclude these 5 trials, K1 was effective in 5 out of 5 trials, even beyond the positive bone markers measured in blood values. One of them throttled the risk of fracture by half,(61) while in two other trials, K1 not only reduced or halted the progression of osteoporosis compared to the placebo but reversed it in both trials by at least 1 measured site!(55,62)
(Even the best result of K2 MK-7 is only a slowing of the progression of osteoporosis, never in any study was it able to stop it, let alone reverse it.)
Placebo-control trials with K2 (MK-4) on bone loss
I found 10 placebo-controlled trials (not counting 3 that were combined with the medication etidronate), of which 1 was ineffective, but that should be ignored as there was no worsening in the placebo group either, so 9/9 were found to be effective, if we look at it generously. In 2-3 trials it had little effect, but in most, it was markedly effective, and like K1, MK-4 was able not only to slow or stop but also to reverse osteoporosis as measured in some areas of the skeleton. Of course, these beneficial effects were shown at supraphysiological doses of at least 45mg, doses below 45mg were found to be ineffective!(63)
Note that in one study, in addition to showing significant improvement in one area, 45mg MK-4 caused increased deterioration compared to placebo when measured at several sites in the hip bone. Is it conceivable that this abnormally high dose could have negative effects in addition to the positive ones? (Quite like in the mouse experiments discussed earlier, where high MK4 upset the tissue ratio and worsened the skeletal condition of the mice, while K1 improved it).(64,33,65,66,54,67,68,69,70,71,72,73,74)
Placebo-controlled studies with K2 (MK-7) on bone loss
It was effective in activating osteocalcin in 4 out of 4 trials, but it affected the bone compared to placebo only in 3 out of 4 trials, although it is true here that where it showed no effect, there was no deterioration in the placebo group, so this result can be excluded. So in 3 out of 3 cases there was an effect, but these effects only reduced the negative change in bone measured at 1 site maximum, they did not stop or reverse it, as was the case for K1 and MK-4 in several trials. In addition, no fracture risk reduction was studied or demonstrated in any of the studies. In addition, in one of the 3 trials comparing K1 with the same dose, K1 was found to be three times more effective than MK-7 in improving spine bone density, with all other effects being equal.(55,75,76,77)
Placebo-controlled studies on the cardiovascular system
In the most recent review/meta-analysis, published in 2020, researchers looked at all placebo-controlled trials to date that lasted more than 3 months using K1 or K2 (MK-7) supplementation and investigating cardiovascular effects. A total of 9 trials were found to be of adequate quality. Of these, three were with vitamin K1 (doses between 200-2000 mcg) and six with K2 (doses between 90-2000 mcg, MK-7). All three K1 trials were found to be effective, while none of the six K2 trials were.(78)
In 6 of the 9 trials, their effect on arterial calcification was investigated. Of these 6 trials, 2 took K1 and 4 took K2. In both K1 trials, K1 was effective in preventing blood vessel calcification. K2 was found to be ineffective in all trials, and in one trial 360 mcg K2 per day even increased calcification compared to a placebo, but we will discuss this more later.
Let's have a look for ourselves, especially as the researchers left out the MK-4 version of K2 from this 2020 review.
Placebo control trials with K1 on the cardiovascular system
In a 3-year study, healthy women aged 50-60 years received 1mg of vitamin K1 daily (along with D3, Ca, Mg and zinc), which helped keep their arteries perfectly healthy. In contrast, those who were given a placebo instead of K1 but received the same combination of D3+Mg+Zn+Ca had a 6-13% increase in blood pressure and fresh calcified plaques, while indicators of artery dilation and condition worsened by 9%. The arteries of those receiving vitamin K1 remained healthy, while those in the groups not receiving K1 aged more rapidly.(79)
Two studies investigated coronary artery calcification. In one, subjects aged 63 years and over received 2mg of K1 per day for 1 year, which is finally an ideal dose. Although 71% of the participants used statin, which impairs the progression of K1->K2, presumably due to the appropriately high K1 dose of 2mg, sufficient K2 was still able to form, as it reduced the progression of their coronary artery calcification by 45% compared to the placebo (those receiving statin alone).(48)
In the other trial, they only received 500 mcg of K1, but at least only 25% used statin, so even this 500 mcg of K1 reduced the progression of coronary atherosclerosis, although in this case by 6% only.(80)
Placebo control studies with K2 (MK-4) on the cardiovascular system
In one study, subjects were given 45mg of K2 daily for 1 year and it proved ineffective in improving or even slowing the deterioration of blood vessels. However, if you excluded data from the severely vitamin K deficient subjects and analyzed the data only in their group, it slowed the deterioration of blood vessel condition by 16% compared to the placebo.(81)
Placebo control studies with K2 (MK-7) one the cardiovascular system
It was ineffective in all studies on the cardiovascular system, although when only the most severe cases from one study were analyzed, a slight effect could be glimpsed. However, in just one of the most recent trials, using a more precise measurement method than previously, it was found that taking 360 mcg K2 MK-7 per day for six months resulted in 10% higher ongoing calcification than placebo. The study participants were diabetic subjects. Such a result was not expected. This study was certainly not sponsored by vitamin K2 manufacturers.
One might think that the problem must be with the new measurement method or that these results were due to the subjects being diabetics. However, a study published in 2021, also in diabetic patients, using the same measurement method, also tested the effect of 10 mg vitamin K1 supplementation on cardiovascular calcification and K1 was found to be very effective: it reduced the risk of calcification by a quarter to a third compared to placebo! (43,44,82,84,90)
In a study published in 2022, K2 mk-7 at a dose of 720 mcg per day supplemented with 1000 IU of vitamin D3 was also ineffective in reducing atherosclerosis, although it is reassuring that at least it did not increase calcification as 360 mcg per day did in diabetics.(83)
These, then, were the placebo-controlled intervention trials that show that vitamin K1 is effective for both skeletal and cardiovascular health, cheap, and effective at doses that can be ingested via food. K2 MK-4 was only effective on skeletal health and only at extremely high supraphysiological doses, although in one study it also showed a negative effect on bone density. In the case of MK-7, nutritionally realistic doses of 100 and 180 mcg were effective on skeletal function, whereas at 360 mcg the effect was reduced and even counterproductive for the arterial system.
Effect of vitamin K on tumors from human studies
Significant cancer risk reduction effects have been observed in both epidemiological and interventional studies using both K1 and K2. In in vitro studies, it has been shown that although each form of vitamin K has different effects on cancer cells, vitamin K3 has the strongest anti-cancer effect due to its ability to induce oxidative stress in cancer cells, generate free radicals and reduce their GSH levels, which lowers their line of defense. In other words, K3 has a cytotoxic effect on cancer cells, but at high doses and in the long run, it is not good for healthy cells, either. Our healthy cells are good at converting K3 to MK-4, so they can't really accumulate K3 -> it can hardly cause issues or be harmful to healthy cells, as is evident from the fact that it is common to enrich animal feed with extremely high K3, still, it is not administered for safety reasons because of the effect mentioned. In any case, it follows that vitamin K1 may be the safest and cheapest form of K3 available, as all K vitamins are converted to vitamin K3 at roughly the same rate, but the utilization of K1 is about 3 times better than MK-4, it is also much cheaper (a tenth of the cost) and K1 alone does not shift the ideal vitamin K ratio for tissues, since neither K2 nor K3 can be converted to K1, whereas K1 is converted to K3->MK-4 and other K2s by gut bacteria in the amounts needed for tissues. Although the utilization of MK-7 is even better, it has proven problematic in a study at 360 mcg and lacks supraphysiological dose studies, so it is not safe in mg doses. In addition, it is 10x more expensive than MK4 and 100x more expensive than K1... High doses of K1 and MK-4 have been safe and shown to have positive effects in both human and animal studies
Anti-cancer or cancer-preventive effects obtained with the use of vitamin K1 in human studies.
There are just a few studies, but in those, it was surprisingly effective:
In a study mentioned above, 440 post-menopausal women were given 5mg of vitamin K1 or placebo daily for 2-4 years and found that it reduced the risk of fracture to less than half, and the risk of cancer to a quarter! Of those in the placebo group, 12 developed cancer, while only 3 of those taking 5mg of K1 had cancer.(85)
In both Phase I and Phase II trials, 2×20mg of vitamin K1 daily was found to be specifically effective in cancer patients: it stabilized the condition, stopped or slowed tumor growth/invasion, and increased survival.(86)
In a 2010 study, patients with advanced, inoperable, metastatic liver cancer were studied. 23 were given 40 mg K1 orally daily, while 27 were given 40-1000 mg intravenously, 1x weekly.
In both groups, 16-16 cases stabilized and 3-3 cases showed a reduction in tumor size. In other words, it helped to stop tumor growth in 70 and 82% of cases, while it induced tumor shrinkage in about 12-15% of cases. This is a very good result and was well tolerated by all patients, with no signs of toxicity.(87)
MK-4-related human studies in cancer
Studies ranged between 20-135mg, mainly 45mg (3x15mg/day), where it has been used in liver cancer patients. Typically, treatment increased survival, slowed progression, and reduced recurrence. While K1 appears to be more effective in the last study mentioned based on these data, there is only one study on the effect of K1 on liver cancer, while there are several for MK-4.(89)
One study reported a case where 45mg MK-4 daily induced complete remission in a leukemia patient.(90)
There are no interventional studies with MK-7 showing a tumor-preventive effect or any studies where it has was used to treat tumors. However, doses in the mg range would be required since it is the conversion to K3 that is responsible for most of the anti-tumor cell effect, so its use can be rejected because it is expensive + as we have seen, starting as low as 0.36 mg it has been shown to cause problems (calcification).
- Saiko IKEDA, Fumiaki HANZAWA, Saki TAKAHASHI, Norie SUZUKI, Kana SANO, Hiroaki ODA, Tomono UCHIDA, Tissue Distribution of Menaquinone-7 and the Effect of α-Tocopherol Intake on Menaquinone-7 Concentration in Rats, Journal of Nutritional Science and Vitaminology, 2018, Volume 64, Issue 6, Pages 391-398, Released December 31, 2018, Online ISSN 1881-7742, Print ISSN 0301-4800, https://doi.org/10.3177/jnsv.64.391
- Jin S, Sell JL. Dietary vitamin K1 requirement and comparison of biopotency of different vitamin K sources for young turkeys. Poult Sci. 2001 May;80(5):615-20. doi: 10.1093/ps/80.5.615. PMID: 11372711.
- Open access peer-reviewed chapter Vitamin K2 in Animal Health: An Overview By Jayde O’Neil, Bethany Scarrott, Ragnhild Aven Svalheim, Jonathan Elliott and Stephen J. Hodges Submitted: January 15th 2016Reviewed: April 22nd 2016Published: March 22nd 2017 DOI: 10.5772/63901
- Open access peer-reviewed chapter Vitamin K2 in Animal Health: An Overview By Jaydn.com/books/vitamin-k2-vital-for-health-and-wellbeing/vitamin-k2-in-animal-health-an-overview
- Hirauchi, K., Sakano, T., Notsumoto, S., Nagaoka, auTadayoshi, Morimoto, A., Fujimoto, K., … Suzuki, Y. (1989). Measurement of k vitamins in animal tissues by high-performance liquid chromatography with fluorimetric detection. Journal of Chromatography B: Biomedical Sciences and Applications, 497, 131–137. doi:10.1016/0378-4347(89)80012-x
- https://www.fda.gov/animal-veterinary/safe-feed/vitamin-k-substances-and-animal-feed
- Schurgers LJ, Vermeer C. (2000) Determination of phylloquinone and menaquinones in food. Effect of food matrix on circulating vitamin K concentrations. Haemostasis. 30(6):298-307
- Koivu-Tikkanen TJ, Ollilainen V, Piironen VI. (2000) Determination of phylloquinone and menaquinones in animal products with fluorescence detection after postcolumn reduction with metallic zinc. Journal of Agriculture and Food Chemistry. 48(12):6325-31.
- Rødbotten, R., Gundersen, T., Vermeer, C., & Kirkhus, B. (2014). Vitamin K2 in different bovine muscles and breeds. Meat Science, 97(1), 49–53. doi:10.1016/j.meatsci.2014.01.005
- https://honey-guide.com/2014/03/10/menaquinones-k2-and-phylloquinone-k1-content-of-animal-products-and-fermented-foods
- Fu, X., Shen, X., Finnan, E. G., Haytowitz, D. B., & Booth, S. L. (2016). Measurement of Multiple Vitamin K Forms in Processed and Fresh-Cut Pork Products in the U.S. Food Supply. Journal of Agricultural and Food Chemistry, 64(22), 4531–4535. doi:10.1021/acs.jafc.6b00938
- J Philip Karl, Mohsen Meydani, Junaidah B Barnett, Sally M Vanegas, Kathryn Barger, Xueyan Fu, Barry Goldin, Anne Kane, Helen Rasmussen, Pajau Vangay, Dan Knights, Satya S Jonnalagadda, Edward Saltzman, Susan B Roberts, Simin N Meydani, Sarah L Booth, Fecal concentrations of bacterially derived vitamin K forms are associated with gut microbiota composition but not plasma or fecal cytokine concentrations in healthy adults, The American Journal of Clinical Nutrition, Volume 106, Issue 4, October 2017, Pages 1052–1061, https://doi.org/10.3945/ajcn.117.155424
- Au, Nicholas T et al. “Dietary Vitamin K and Association with Hepatic Vitamin K Status in a Yup’ik Study Population from Southwestern Alaska.” Molecular nutrition & food research vol. 62,3 (2018): 10.1002/mnfr.201700746. doi:10.1002/mnfr.201700746
- Eaton SB, Eaton SB 3rd, Konner MJ. Paleolithic nutrition revisited: a twelve-year retrospective on its nature and implications. Eur J Clin Nutr. 1997 Apr;51(4):207-16. doi: 10.1038/sj.ejcn.1600389. PMID: 9104571. ] [Loren Cordain: The Nutritional Characteristics of a Contemporary Diet Based Upon Paleolithic Food Groups, JANA Vol. 5, No. 3 Summer 2002 https://thepaleodiet.com/wp-content/uploads/2015/08/The-Nutritional-Characteristics-of-a-Contemporary-Diet-Based-Upon-Paleolithic-Food-Groups-The-Paleo-Diet.pdf
- Simes DC, Viegas CSB, Araújo N, Marreiros C. Vitamin K as a Diet Supplement with Impact in Human Health: Current Evidence in Age-Related Diseases. Nutrients. 2020;12(1):138. Published 2020 Jan 3. doi:10.3390/nu12010138
- Thijssen HH, Drittij-Reijnders MJ. Vitamin K status in human tissues: tissue-specific accumulation of phylloquinone and menaquinone-4. Br J Nutr. 1996 Jan;75(1):121-7. doi: 10.1079/bjn19960115. PMID: 8785182.
- Fu, X., Moreines, J. & Booth, S.L. Vitamin K supplementation does not prevent bone loss in ovariectomized Norway rats. Nutr Metab (Lond) 9, 12 (2012). https://doi.org/10.1186/1743-7075-9-12
- Yamaguchi, M., Taguchi, H., Gao, Y. H., Igarashi, A., & Tsukamoto, Y. (1999). Effect of vitamin K 2 (menaquinone-7) in fermented soybean ( natto ) on bone loss in ovariectomized rats. Journal of Bone and Mineral Metabolism, 17(1), 23–29. doi:10.1007/s007740050059
- Sato T, Kawahara R, Kamo S, Saito S. Comparison of menaquinone-4 and menaquinone-7 in rats. Vitamins (Japan) 2007;81:377–381.
- Okano T, Shimomura Y, Yamane M, Suhara Y, Kamao M, Sugiura M, Nakagawa K. Conversion of phylloquinone (Vitamin K1) into menaquinone-4 (Vitamin K2) in mice: two possible routes for menaquinone-4 accumulation in cerebra of mice. J Biol Chem. 2008 Apr 25;283(17):11270-9. doi: 10.1074/jbc.M702971200. Epub 2007 Dec 14. PMID: 18083713
- Hirota Y, Tsugawa N, Nakagawa K, et al. Menadione (vitamin K3) is a catabolic product of oral phylloquinone (vitamin K1) in the intestine and a circulating precursor of tissue menaquinone-4 (vitamin K2) in rats. J Biol Chem. 2013;288(46):33071-33080. doi:10.1074/jbc.M113.477356
- Ala Al Rajabi, Sarah L. Booth, James W. Peterson, Sang Woon Choi, John W. Suttie, M. Kyla Shea, Benchun Miao, Michael A. Grusak, Xueyan Fu, Deuterium-Labeled Phylloquinone Has Tissue-Specific Conversion to Menaquinone-4 among Fischer 344 Male Rats, The Journal of Nutrition, Volume 142, Issue 5, May 2012, Pages 841–845, https://doi.org/10.3945/jn.111.155804 – Megj.: „In conclusion, MK-4 is the predominant form of vitamin K in multiple tissues, but there appears to be a tissue-specific regulation for the conversion of PK to MK-4. To convert PK to MK-4, the phytyl side chain in PK is removed and a geranylgeranyl side chain is added to the MD nucleus, forming MK-4. However, our data do not support the involvement of enterocytes in this conversion.”
- Nakagawa K, Hirota Y, Sawada N, Yuge N, Watanabe M, Uchino Y, Okuda N, Shimomura Y, Suhara Y, Okano T. Identification of UBIAD1 as a novel human menaquinone-4 biosynthetic enzyme. Nature. 2010 Nov 4;468(7320):117-21. doi: 10.1038/nature09464. Epub 2010 Oct 17. PMID: 20953171.
- Shearer MJ, Fu X, Booth SL. Vitamin K nutrition, metabolism, and requirements: current concepts and future research. Adv Nutr. 2012;3(2):182-195. Published 2012 Mar 1. doi:10.3945/an.111.001800 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3648719 – Megj.:„ (UBIAD1) that Nakagawa et al. (60) proposed not only catalyzed the well-described prenylation of precursor menadione to MK-4 but might also be responsible for the initial side chain cleavage of phylloquinone or other MK.”
- https://chrismasterjohnphd.com/blog/2009/04/07/tufts-university-confirms-that-vitamin
- Fu X, Wang XD, Mernitz H, Wallin R, Shea MK, Booth SL. 9-Cis retinoic acid reduces 1alpha,25-dihydroxycholecalciferol-induced renal calcification by altering vitamin K-dependent gamma-carboxylation of matrix gamma-carboxyglutamic acid protein in A/J male mice. J Nutr. 2008 Dec;138(12):2337-41. doi: 10.3945/jn.108.093724. PMID: 19022954.
- Yamaguchi M, Kakuda H, Gao YH, et al. Prolonged intake of fermented soybean (natto) diets containing vitamin K2 (menaquinone-7) prevents bone loss in ovariectomized rats. J Bone Miner Metab. 2000;18(2): 71–76.
- Craciun AM, Wolf J, Knapen MH, Brouns F, Vermeer C. Improved bonemetabolism in female elite athletes after vitamin K supplementation. Int J Sports Med. 1998;19(7):479–484. PubMed PMID: 9839845.
- Schurgers LJ, Spronk HM, Soute BA, et al. Regression of warfarin-induced medial elastocalcinosis by high intake of vitamin K in rats. Blood. 2007;109(7):2823–2831.
- Spronk HM, Soute BA, Schurgers LJ, et al. Tissue-specific utilization of menaquinone-4 results in the prevention of arterial calcification in warfarin-treated rats. J Vasc Res. 2003;40(6):531–537
- Thijssen et al: Menadione is a metabolite of oral vitamin K. British Journal of Nutrition (2006), 95, 260–266
- Thijssen HH, Drittij MJ, Vermeer C, Schoffelen E. Menaquinone-4 in breast milk is derived from dietary phylloquinone. Br J Nutr. 2002 Mar;87(3):219-26. doi: 10.1079/BJNBJN2001505. PMID: 12064330.
- Koitaya, N., Sekiguchi, M., Tousen, Y., Nishide, Y., Morita, A., Yamauchi, J., … Ishimi, Y. (2013). Low-dose vitamin K2 (MK-4) supplementation for 12 months improves bone metabolism and prevents forearm bone loss in postmenopausal Japanese women. Journal of Bone and Mineral Metabolism, 32(2), 142–150. doi:10.1007/s00774-013-0472-7
- Inaba N, Sato T, Yamashita T. Low-Dose Daily Intake of Vitamin K(2) (Menaquinone-7) Improves Osteocalcin γ-Carboxylation: A Double-Blind, Randomized Controlled Trials. J Nutr Sci Vitaminol (Tokyo). 2015;61(6):471-80. doi: 10.3177/jnsv.61.471. PMID: 26875489.
- Funahashi N, Hirota Y, Nakagawa K, Swada N, Watanabe M, Suhara Y, Okano T. YY1 positively regulates human UBIAD1 expression. Biochem Biophys Res Commun. 2015 May 1;460(2):238-44. doi: 10.1016/j.bbrc.2015.03.018. Epub 2015 Mar 12. PMID: 25772619.
- Hirota Y, Nakagawa K, Sawada N, Okuda N, Suhara Y, Uchino Y, Kimoto T, Funahashi N, Kamao M, Tsugawa N, Okano T. Functional characterization of the vitamin K2 biosynthetic enzyme UBIAD1. PLoS One. 2015 Apr 15;10(4):e0125737. doi: 10.1371/journal.pone.0125737. PMID: 25874989; PMCID: PMC4398444.
- Schurgers LJ, Teunissen KJ, Hamulyák K, Knapen MH, Vik H, Vermeer C. Vitamin K-containing dietary supplements: comparison of synthetic vitamin K1 and natto-derived menaquinone-7. Blood. 2007 Apr 15;109(8):3279-83. doi: 10.1182/blood-2006-08-040709. Epub 2006 Dec 7. PMID: 17158229
- Takeuchi, A., et al. “Minimal effective dose of vitamin K2 (menaquinone-4) on serum osteocalcin concentration in Japanese subjects and safety evaluation of vitamin K2 supplemented in calcium tablet.” J Jpn Soc Clin Nutr 26 (2005): 254-260.
- Sato, Toshiro et al. “Comparison of menaquinone-4 and menaquinone-7 bioavailability in healthy women.” Nutrition journal vol. 11 93. 12 Nov. 2012, doi:10.1186/1475-2891-11-93.
- Nakamura E, Aoki M, Watanabe F, Kamimura A. Low-dose menaquinone-4 improves γ-carboxylation of osteocalcin in young males: a non-placebo-controlled dose-response study. Nutr J. 2014 Aug 27;13:85. doi: 10.1186/1475-2891-13-85. PMID: 25163392; PMCID: PMC4155127.
- Schurgers LJ, Vermeer C. Differential lipoprotein transport pathways of K-vitamins in healthy subjects. 2002; 1570: 27-32.
- Binkley NC, Krueger DC, Kawahara TN, et al. A high phylloquinone intake is required to achieve maximal osteocalcin gamma-carboxylation. Am J Clin Nutr. 2002;76(5):1055–1060.
- Knapen MH, Braam LA, Drummen NE, Bekers O, Hoeks AP, Vermeer C. Menaquinone-7 supplementation improves arterial stiffness in healthy postmenopausal women. A double-blind randomised clinical trial. Thromb Haemost. 2015;113(5):1135–1144. https://doi.org/10.1160/ TH14-08-0675. Epub 2015 Feb 19. PubMed PMID: 25694037.
- Fulton RL, McMurdo ME, Hill A, et al. Effect of vitamin K on vascular health and physical function in older people with vascular disease—a randomised controlled trial. J Nutr Health Aging. 2016;20(3):325–333. https://doi.org/10.1007/s12603-015-0619 PubMed PMID: 26892582.
- Theuwissen E, Cranenburg EC, Knapen MH, et al. Low-dose menaquinone-7 supplementation improved extra-hepatic vitamin K status, but had no effect on thrombin generation in healthy subjects. Br J Nutr. 2012;108(9):1652–1657. https://doi.org/10.1017/S0007114511007185. Epub 2012 Jan 31. PubMed PMID: 22289649.]
- Shea MK, O’Donnell CJ, Vermeer C, et al. Circulating uncarboxylated matrix gla protein is associated with vitamin K nutritional status, but not coronary artery calcium, in older adults. J Nutr. 2011;141(8):1529–1534. https://doi.org/10.3945/jn.111.139634 Epub 2011 May 31. PubMed PMID: 21628633; PubMed Central PMCID: PMC3138643.]
- Dalmeijer GW, van der Schouw YT, Magdeleyns E, Ahmed N, Vermeer C, Beulens JW. The effect of menaquinone-7 supplementation on circulating species of matrix Gla protein. Atherosclerosis. 2012;225(2):397–402. https://doi.org/10.1016/j.atherosclerosis.2012.09.019 Epub 2012 Sep 25. PubMed PMID: 23062766]
- Brandenburg VM, Reinartz S, Kaesler N, et al. Slower progress of aortic valve calcification with vitamin K supplementation: results from a prospective interventional proof-of-concept study. Circulation. 2017;135(21):2081–2083. https://doi.org/10.1161/CIRCULATIONAHA.116.027011 PubMed PMID: 28533322.]
- Joyce C McCann, Bruce N Ames, Vitamin K, an example of triage theory: is micronutrient inadequacy linked to diseases of aging?, The American Journal of Clinical Nutrition, Volume 90, Issue 4, October 2009, Pages 889–907, https://doi.org/10.3945/ajcn.2009.27930
- Geleijnse JM, Vermeer C, Grobbee DE, Schurgers LJ, Knapen MH, van der Meer IM, Hofman A, Witteman JC: Dietary intake of menaquinone is associated with a reduced risk of coronary heart disease: the Rotterdam Study. J Nutr. 2004 Nov; 134(11): 3100-3105.
- Beulens JW, Bots ML, Atsma F, Bartelink ML, Prokop M, Geleijnse JM, Witteman JC, Grobbee DE, van der Schouw YT. High dietary menaquinone intake is associated with reduced coronary calcification. Atherosclerosis. 2009 Apr;203(2):489-93.
- Erkkilä AT, Booth SL, Hu FB, et al. Phylloquinone intake as a marker for coronary heart disease risk but not stroke in women. Eur J Clin Nutr. 2005;59(2):196–204. PubMed PMID: 15454972)
- Juanola-Falgarona M, Salas-Salvadó J,et. al. Dietary intake of vitamin K is inversely associated with mortality risk. J Nutr. 2014;144(5):743–750. https://doi.org/10.3945/jn.113.187740. Epub 2014 Mar 19. Erratum in: J Nutr. 2016 Mar;146(3):653. PubMed PMID: 24647393
- Binkley N, Harke J, Krueger D, et al. Vitamin K treatment reduces undercarboxylated osteocalcin but does not alter bone turnover, density,or geometry in healthy postmenopausal North American women. J Bone Miner Res. 2009;24(6):983–991
- Kanellakis S, Moschonis G, Tenta R, et al. Changes in parameters of bone metabolism in postmenopausal women following a 12-month intervention period using dairy products enriched with calcium, vitamin D, and phylloquinone (vitamin K(1)) or menaquinone-7 (vitamin K (2)): the Postmenopausal Health Study II. Calcif Tissue Int. 2012;90(4):251–262. https://doi.org/10.1007/s00223-012-9571-z Epub 2012 Mar 4. PubMed PMID: 22392526.
- Iwamoto et al.: High-dose vitamin K supplementation reduces fracture incidence in postmenopausal women: a review of the literature. Nutrition Research 29 (2009) 221–228
- Hao G, Zhang B, Gu M, et al. Vitamin K intake and the risk of fractures: A meta-analysis. Medicine (Baltimore). 2017;96(17):e6725. doi:10.1097/MD.0000000000006725
- Shea MK, Dallal GE, Dawson-Hughes B, et al. Vitamin K, circulating cytokines, and bone mineral density in older men and women. Am J Clin Nutr. 2008;88(2):356–363.
- Walther B, Karl JP, Booth SL, Boyaval P. Menaquinones, bacteria, and the food supply: the relevance of dairy and fermented food products to vitamin K requirements.
- Braam LA, Knapen MH, Geusens P, Brouns F, Vermeer C. Factors affecting bone loss in female endurance athletes: a two-year follow-up study. Am J Sports Med. 2003;31(6):889–895. PubMed PMID: 14623654.
- Sato Y, Nakamura R, Satoh M, et al. Thyroid hormone targets matrix Gla protein gene associated with vascular smooth muscle calcification. Circ Res. 2005;97(6):550–557.
- Harshman SG, Saltzman E, Booth SL. Vitamin K: dietary intake and requirements in different clinical conditions. Curr Opin Clin Nutr Metab Care. 2014;17(6):531–538. https://doi.org/10.1097/MCO.0000000000000112. Review. PubMed PMID: 25232640
- Iwamoto J, Sato Y. Menatetrenone for the treatment of osteoporosis. Expert Opin Pharmacother. 2013 Mar;14(4):449-58. doi: 10.1517/14656566.2013.763796. Epub 2013 Jan 25. Retraction in: Expert Opin Pharmacother. 2019 Aug;20(12):1531. PMID: 23346882.]
- Knapen MH, Schurgers LJ, Vermeer C. Vitamin K2 supplementation improves hip bone geometry and bone strength indices in postmenopausal women. Osteoporos Int. 2007;18(7):963–972.
- Ushiroyama T, Ikeda A, Ueki M. Effect of continuous combined therapy with vitamin K(2) and vitamin D(3) on bone mineral density and coagulofibrinolysis function in postmenopausal women. Maturitas. 2002;41(3):211–221.
- Orimo H, Shiraki M, Tomita A, Morii H, Fujita T, Ohata M. Effects of menatetrenone on the bone and calcium metabolism in osteoporosis: a double‐ blind placebo‐controlled study. J Bone Miner Metab, 1998. 16: 106–112.: Megj.: napi 90 mg nem csak lassítani vagy megállítani tudta, de vissza is fordítani a csontritkulást (+2% BMD). 80 fő
- Shiraki M, Shiraki Y, Aoki C, Miura M . Vitamin K2 ( menatetrenone) effectively prevents fracture and sustains lumbar bone mineral density in osteoporosis. J Bone Miner Res, 2000. 15: 515–521. Megj.: Bár BMD-t nem tudta növelni, de töréskockázatot kb felére csökkentette
- Iwamoto J, Takeda T, Ichinura S. Effect of combined administration of vitamin D3 and vitamin K2 on bone mineral density of the lumbar spine in postmenopausal women with osteoporosis. J Orthop Sci, 2000. 5: 546–551.
- Iwamoto J, Takeda T, Ichmura S. Treatment with vitamin D3 and/or vitamin K2 for postmenopausal osteoporosis. Keio J Med, 2003. 52: 147–150.
- Iwamoto J, Takeda T, Ichimura S. Effect of menatetrenone on bone mineral density and incidence of vertebral fractures in postmenopausal women with osteoporosis: a comparison with the effect of etidronate. J Orthop Sci. 2001; 6(6): 487–492. Megj.: Nem csökkentette töréskockázatot, BMD-t enyhén mérsékelte, de nem növelte
- Iwamoto J, Takeda T, Ishmura S. Combined treatment with K2 and bisphosphonate in postmenopausal women with osteoporosis. Yonsei Med J, 2003. 44: 751-756. Megj.: Etidronate gyógyszerrel együtt az MK-4 hatásosabban fokozta BMD-t, mint az etidronate külön. Önmagában az MK-4 nem fokozta, de segített lassítani a romlását.
- Iwamoto J. Vitamin K2 therapy for postmenopausal osteoporosis. Nutrients, 2014. 6: 1971–1980. Megj.: Etidronate gyógyszerrel együtt az MK-4 hatásosabban fokozta BMD-t, mint az etidronate külön. Önmagában az MK-4 nem fokozta, de segített lassítani a romlását.
- Ishida Y and Kawai S. Comparative efficacy of hormone replacement therapy, etidronate, calcitonin, alfacalcidol, and vitamin K in postmenopausal women with osteoporosis: The Yamaguchi Osteoporosis Prevention Study. Am J Med, 2004. 117(8): 549–555.: Megj.:Etidronatenál kevésbé, de így is kb felére csökk törés kock.
- Je SH, Joo NS, Choi B h, Kim KM, Kim BT, Park SB, Cho DY, Kim KN, Lee DJ. Vitamin K supplement along with vitamin D and calcium reduced serum concentration of undercarboxylated osteocalcin while increasing bone mineral density in Korean postmenopausal women over sixty years old. J Korean Med Sci, 2011. 26(8): 1093–1098. Megj.:Enyhe hatás 4-ből 1helyen javított BMD-n, máshol nem.
- Emaus N, Gjesdal CG, Almås B, et al. Vitamin K2 (MK-7) supplementation does not influence bone loss in early menopausal women: a randomised double-blind placebo-controlled trial. Osteoporos Int. 2010;21(10):1731–1740. https://doi.org/10.1007/s00198-009-1126-4. Epub 2009 Nov 25. PubMed PMID: 19937427.
- Knapen MH, Drummen NE, Smit E, Vermeer C, Theuwissen E. Threeyear low-dose menaquinone-7 supplementation helps decrease bone loss in healthy postmenopausal women. Osteoporos Int. 2013;24(9):2499– https://doi.org/10.1007/s00198-013-2325-6. Epub 2013 Mar 23. PubMed PMID: 23525894.
- Rønn SH, Harsløf T, Pedersen SB, Langdahl BL. Vitamin K2 (menaquinone-7) prevents age-related deterioration of trabecular bone microarchitecture at the tibia in postmenopausal women. Eur J Endocrinol. 2016;175(6):541–549. Epub 2016 Sep 13. PubMed PMID: 27625301.
- Vlasschaert C, Goss CJ, Pilkey NG, McKeown S, Holden RM. Vitamin K Supplementation for the Prevention of Cardiovascular Disease: Where Is the Evidence? A Systematic Review of Controlled Trials. Nutrients. 2020;12(10):2909. Published 2020 Sep 23. doi:10.3390/nu12102909 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7598164/
- Braam LA, Hoeks AP, Brouns F, et al. Beneficial effects of vitamins D and K on the elastic properties of the vessel wall in postmenopausal women: a follow-up study. Thromb Haemost. 2004;91(2):373–380.
- Shea MK, O’Donnell CJ, Hoffmann U, et al. Vitamin K supplementation and progression of coronary artery calcium in older men and women. Am J Clin Nutr. 2009;89(6):1799–1807.
- Ikari Y, Torii S, Shioi A, Okano T. Impact of menaquinone-4 supplementation on coronary artery calcification and arterial stiffness: an open label single arm study. Nutr J. 2016;15(1):53. https://doi.org/10.1186/s12937-016-
- Zwakenberg SR, de Jong PA, Bartstra JW, et al. The effect of menaquinone-7 supplementation on vascular calcification in patients with diabetes: a randomized, double-blind, placebo-controlled trial. Am J Clin Nutr. 2019;110(4):883–890. https://doi.org/10.1093/ajcn/nqz147.
- Diederichsen ACP, Lindholt JS, Möller S, Øvrehus KA, Auscher S, Lambrechtsen J, Hosbond SE, Alan DH, Urbonaviciene G, Becker SW, Fredgart MH, Hasific S, Folkestad L, Gerke O, Rasmussen LM, Møller JE, Mickley H, Dahl JS. Vitamin K2 and D in Patients With Aortic Valve Calcification: A Randomized Double-Blinded Clinical Trial. Circulation. 2022 May 3;145(18):1387-1397. doi: 10.1161/CIRCULATIONAHA.121.057008. Epub 2022 Apr 25. PMID: 35465686; PMCID: PMC9047644.
- Jamie W Bellinge, Roslyn J Francis, Sing C Lee, Nicola P Bondonno, Marc Sim, Joshua R Lewis, Gerald F Watts, Carl J Schultz, The effect of vitamin K1 on arterial calcification activity in subjects with diabetes mellitus: a post hoc analysis of a double-blind, randomized, placebo-controlled trial, The American Journal of Clinical Nutrition, 2021;, nqab306, https://doi.org/10.1093/ajcn/nqab306
- Cheung AM, Tile L, Lee Y, Tomlinson G, Hawker G, Scher J, Hu H, Vieth R, Thompson L, Jamal S, Josse R. Vitamin K supplementation in postmenopausal women with osteopenia (ECKO trial): a randomized controlled trial. PLoS Med. 2008 Oct 14;5(10):e196. doi: 10.1371/journal.pmed.0050196. Erratum in: PLoS Med. 2008 Dec;5(12):e247. PMID: 18922041; PMCID: PMC2566998.
- Lamson DW, Plaza SM. The anticancer effects of vitamin K. Altern Med Rev. 2003;8(3):303–318. Review.
- Carr BI, Wang Z, Wang M, et al. Differential effects of vitamin K1 on AFP and DCP levels in patients with unresectable HCC and in HCC cell lines. Dig Dis Sci. 2010.
- Mizuta T, Ozaki I, Eguchi Y, et al. The effect of menatetrenone, a vitamin K2 analog, on disease recurrence and survival in patients with hepatocellular carcinoma after curative treatment: a pilot study. Cancer. 2006;106(4):867–872.]
- Abe Y, Muta K, Hirase N, et al. Vitamin K2 therapy for myelodysplastic syndrome. Rinsho Ketsueki. 2002;43(2):117–121
- Bartstra JW, Draaisma F, Zwakenberg SR, Lessmann N, Wolterink JM, van der Schouw YT, de Jong PA, Beulens JWJ. Six months vitamin K treatment does not affect systemic arterial calcification or bone mineral density in diabetes mellitus 2. Eur J Nutr. 2021 Apr;60(3):1691-1699. doi: 10.1007/s00394-020-02412-z. Epub 2020 Oct 17. PMID: 33068157; PMCID: PMC7987615.